NYS Heavy Metals Registry, 2010-2015
- This report, New York State Heavy Metals Registry, 2010 through 2015, is available in Portable Document Format (PDF, 640KB).
The New York State Department of Health (NYSDOH) Heavy Metals Registry (HMR) is a tool for the surveillance of adult exposures to arsenic, cadmium, lead and mercury. These metals are widely used in industry, and all have the potential to cause illness due to either acute or chronic exposure. While heavy metals have been used by humans for thousands of years and the adverse health effects associated with exposure to them are well known, exposure to these metals continues. Examination of the Registry data can identify exposures in both communities and workplaces, thus allowing for early initiation of measures to help prevent exposures and potential illness.
| Metal | Sample | Reportable At or Above |
|---|---|---|
| Lead | Blood | All levels |
| Cadmium | Blood | 10 nanograms per milliliter |
| Urine | 5 micrograms per liter | |
| Mercury | Blood | 5 nanograms per milliliter |
| Urine | 20 nanograms per milliliter | |
| Arsenic | Urine | 50 micrograms per liter |
The NYSDOH established the HMR in 1980 under Sections 22.6 and 22.7 of the State Sanitary Code (10 NYCRR Part 22, see Appendix A), and reporting to the Registry began in 1982. All clinical laboratories, physicians and health care facilities, both in-state and out of NYS must report the test results of all NYS residents to the NYSDOH. For mercury, cadmium and arsenic, only those tests above specified limits (Table 1) are required to be submitted to NYSDOH. From 1982 to 1986, blood lead levels of 40 micrograms per deciliter (µg/dL) or higher were reportable. In 1986, the reportable blood lead level was lowered to 25 µg/dL or higher. Then in 1992, as part of a major childhood lead poisoning initiative, a regulatory change required the reporting of all blood lead results for all age groups, regardless of level (10 NYCRR Part 67, see Appendix A). This reporting has helped track adult blood lead levels over time by verifying trends in both individuals and companies and has allowed NYSDOH to proactively identify adults potentially at risk before their blood lead levels increase further.
Clinical laboratories, physicians and health care facilities report heavy metal test results to the NYSDOH. Once information is received on a person with an elevated level, NYSDOH contacts the person and/or their physician and interviews them to determine the possible sources of exposure, provide advice on appropriate measures to limit future exposures to the individual and his or her family, and answer any questions the individual may have. Additional information about how the HMR operates is provided in Appendix B.
This report presents data for tests conducted from 2006 through 2010, and covers the four metals included in the HMR – arsenic, cadmium, lead and mercury. The number of adults reported since the inception of the Registry is presented for each metal. This report is intended as a resource for programs providing preventive health care and for public health officials concerned with reducing overall morbidity from heavy metals poisonings. Because of the change in the reporting requirement for lead in 1992 and because testing for lead exposure among adults is much more common, lead tests account for approximately 75 percent of the tests added to the HMR each year. Therefore, the majority of this report focuses on the lead reports.
Arsenic
Arsenic is a naturally occurring chemical element. In the environment, it combines with oxygen, chlorine and sulfur to form inorganic arsenic compounds. Inorganic arsenic compounds are used in a number of industrial processes such as in the making of electronics. Fish and shellfish accumulate arsenic, most of which is in a relative non-toxic organic form.1
Exposure to high levels of inorganic arsenic can cause death; exposure to lower levels can result in nausea and vomiting, decreased production of red and white blood cells, abnormal heart rhythm, damage to blood vessels, darkening of the skin and the appearance of small "warts" on the palms, soles and torso. Inorganic arsenic is also a known carcinogen.2
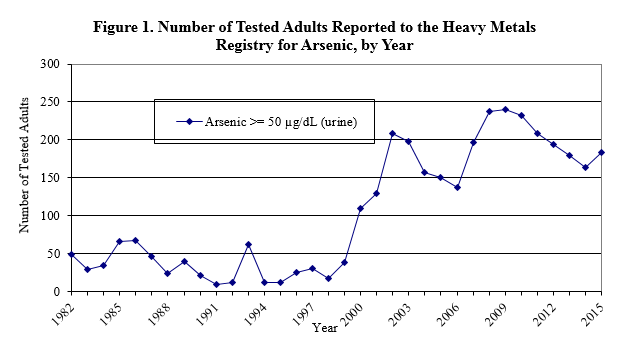
From 1982 through 1999, the number of adults reported to the Registry for arsenic each year was, with a few exceptions, below 50. In 2000, 111 adults were reported. Since then, the number of adults reported continued to vary but remained above 100, increasing to a high of 244 adults in 2010, before beginning to gradually decline. This rise is most likely because of an increase in the number of people tested due to greater public awareness that exposure to heavy metals is possible through seafood consumption.
During the years 2010-2015, 56 percent of the adults reported to the HMR for arsenic were male, and over 60 percent were 50 years of age or older (Table 2). For 55 percent of the adults reported, the exposure source was non-occupational; however, the source could not be identified for another 44 percent. In general, however non-occupational sources of arsenic exposure are attributed to eating seafood; over 99.5 percent of the known sources of non-occupational exposure were due to eating seafood, with a few adults exposed to arsenic through the use of folk medicine and dietary supplements. Because most laboratories do not routinely distinguish between organic and inorganic forms of arsenic when they test, NYSDOH advises people with elevated arsenic results to avoid seafood consumption for two days prior to testing and have another test. This can help to indicate if seafood was the source of the initial arsenic level. There were approximately 1.13 tests reported for each adult, indicating that people with reportable levels are either not being routinely retested, or if they are being retested, their arsenic levels are falling below the reporting level of 50 µg/dL. NYSDOH does not advise routine testing of individuals for arsenic in the absence of identifiable risk factors.
| Number of Adults | N | % |
|---|---|---|
| 1,157 | ||
| Sex | ||
| Male | 653 | 56.4 |
| Female | 504 | 43.6 |
| Age | ||
| <29 years | 109 | 9.4 |
| 30-49 years | 329 | 28.4 |
| >50 years | 719 | 62.2 |
| Exposure | ||
| Occupational | 8 | 0.7 |
| Non-occupational | 636 | 55.0 |
| Both | 7 | 0.6 |
| Unknown | 485 | 43.7 |
| Geographic Area | ||
| NYS w/o NYC | 744 | 64.3 |
| NYC | 381 | 32.9 |
| Not in NYS | 27 | 2.3 |
| Total Number of Tests* | 1,303 | |
| * The number of tests adds up to more than the number of adults because adults can have multiple arsenic tests. | ||
Cadmium
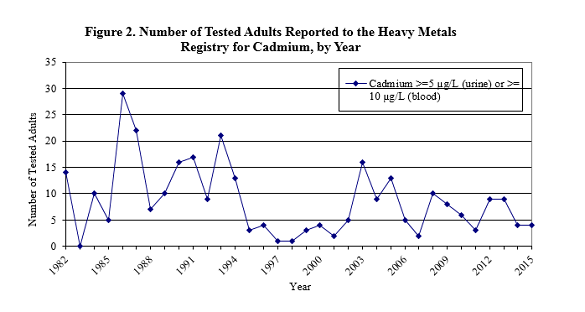
Cadmium occurs naturally in soil and rocks. Because it does not corrode easily, it has many uses including batteries, pigments, metal coatings and plastics.3 Exposure to cadmium can damage the kidneys, lungs and bones.4 Cadmium levels of 10 nanograms per milliliter (ng/mL) in blood and 5 µg/L in urine are reportable to NYSDOH. The number of adults with reportable levels for cadmium has varied considerably since the Registry began (Figure 2). However, there have always been fewer than 30 adults reported to the HMR each year. NYSDOH does not advise routine testing for cadmium in the absence of identifiable risk factors.
Between 2010 and 2015, there were 36 adults with elevated cadmium levels reported to the HMR (Table 3). Approximately two-thirds of those reported were male, and more than 60 percent resided outside of New York City (NYC). Four individuals had known occupational exposures, most of whom were involved in smelter work. Eight people were exposed to cadmium non-occupationally, through unspecified environmental sources. The exposure source could not be identified for eighteen individuals, and over 80 percent of these individuals were not interviewed after repeated attempts were made. Thus, detailed exposure information could not be obtained.
| Number of Adults | N | % |
|---|---|---|
| 36 | ||
| Sex | ||
| Male | 23 | 63.9 |
| Female | 13 | 36.1 |
| Age | ||
| <29 years | 4 | 11.1 |
| 30-49 years | 17 | 47.2 |
| >50 years | 15 | 41.7 |
| Exposure | ||
| Occupational | 8 | 19.4 |
| Non-occupational | 9 | 25.0 |
| Both | 2 | 5.6 |
| Unknown | 18 | 50.0 |
| Geographic Area | ||
| NYS w/o NYC | 22 | 61.1 |
| NYC | 9 | 25.0 |
| Not in NYS/Unknown | 5 | 13.9 |
| Total Number of Tests* | 53 | |
| * The number of tests adds up to more than the number of adults because adults can have multiple cadmium tests. | ||
Lead
Lead, a naturally occurring element, is found in all parts of our environment. Lead from deteriorating lead-based paints, ceramic products, caulking, leaded gasoline and pipe solder are primarily responsible for exposures in children. Workers can be exposed to lead by creating dust or fumes during every day work activities with products that include lead, such as paint, ammunition, solder, and leaded cables. Other non-occupational exposures can include contaminated spices and dietary supplements. Exposure to lead can affect the brain and other parts of the nervous system, reproductive system, kidneys, digestive system, and the body's ability to make blood.5
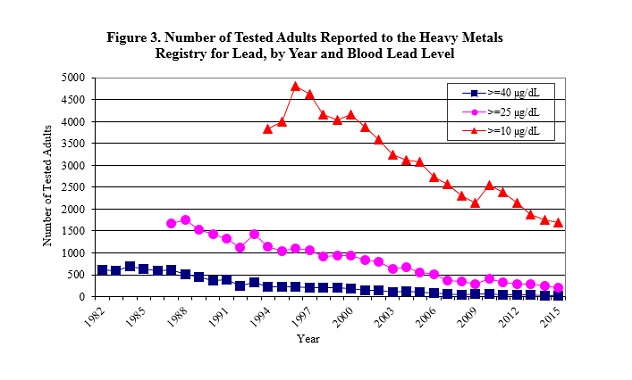
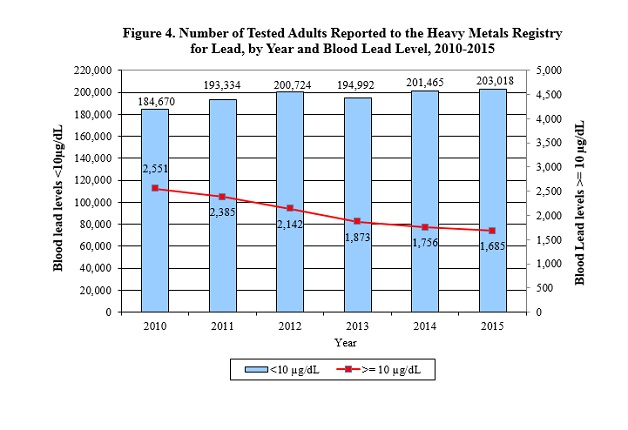
The results of all blood lead tests, regardless of level, performed on individuals residing or employed in NYS are reported to the HMR. Between 2010 and 2015, 7,517 individuals residing or employed in NYS were reported to the HMR. There was a steady decrease in the number of elevated blood lead levels reported to the HMR since the mid-1990's (Figure 3), until 2010 when a slight increase was observed. Although the total number of blood lead tests has increased since 2010, there has been an overall decrease in the number of individuals with elevated blood lead levels (Figure 4). Approximately 98.6 percent of all adults tested in 2010 had blood lead levels less than 10 µg/d, assuming one test per individual for those tests that are less than 10 µg/dL. In 2015, this increased to 99.2 percent of all adults tested.
Females represented over 80 percent of those adults with blood lead levels less than 10 µg/dL (data not shown). Although NYS does not require testing all pregnant women for blood lead, NYSDOH regulations state that a health care provider should test pregnant women at high risk, and the state has established guidelines for health care practitioners to assist in determining a woman's risk of lead poisoning on her initial prenatal visit.7 The high number of females with low blood lead levels could be a result of an increase in women receiving pre-natal blood lead tests.
In general, tested adults with blood lead levels 10 µg/dL and greater reported to the HMR between 2010 and 2015 were primarily males 30 to 49 years of age, and approximately half resided in NYS outside of NYC (Table 4). Although approximately 80 percent of those reported are male, gender distribution varies by blood lead level (Table 5). Twenty percent of those with blood lead levels (between 10 and 24 µg/dL) and 24 percent of those with the highest blood lead levels (60 µg/dL and greater) are female. The highest blood lead levels among females were all associated with non-occupational exposures (data not shown). Almost 70 percent of the tested adults with unknown exposures were not interviewed because they could not be contacted after repeated attempts were made. Thus, detailed exposure information could not be obtained.
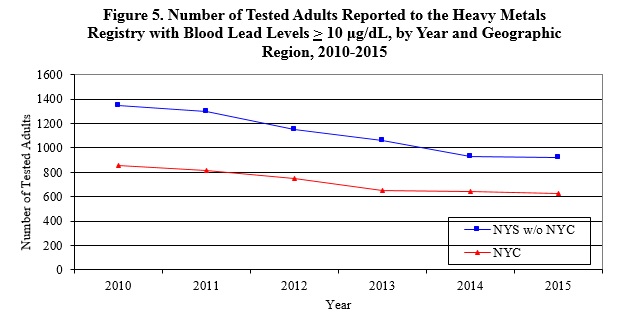
Changes in the number of people reported to the HMR from 2010 through 2015 are similar for NYC and the rest of the state (Figure 5). The change in blood lead levels from 2010 through 2015 is similar for those in NYC and those in the rest of the state (Figure 5).
| Number of Adults | N | % |
|---|---|---|
| 7,517 | ||
| Sex | ||
| Male | 6,066 | 80.7 |
| Female | 1,451 | 19.3 |
| Age | ||
| <29 years | 1,792 | 24.0 |
| 30-49 years | 3,709 | 49.3 |
| >50 years | 2,016 | 26.7 |
| Unknown | 3 | 0 |
| Exposure | ||
| Occupational | 3,219 | 42.8 |
| Non-Occupational | 1,197 | 15.9 |
| Both | 213 | 2.8 |
| Unknown | 2,888 | 38.4 |
| Geographic Area | ||
| NYS w/o NYC | 3,956 | 52.6 |
| NYC | 2,782 | 37.0 |
| Out of state | 700 | 9.3 |
| Unknown | 79 | 1.1 |
| Total Number of Tests* | 26,013 | |
| * The number of tests adds up to more than the number of adults because adults can have multiple lead tests. | ||
| Tested Adults | Peak Blood Lead Levels (µg/dL) | Total | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 10-24 | 25-39 | 40-59 | 60+ | |||||||||
| N | %* | N | %* | N | %* | N | %* | N | %* | |||
| 6,201 | 1,085 | 202 | 29 | 7,517 | ||||||||
| Sex | ||||||||||||
| Male | 4,929 | 79.5 | 948 | 87.4 | 167 | 82.7 | 22 | 75.9 | 6,066 | 80.7 | ||
| Female | 1,272 | 20.5 | 137 | 12.6 | 35 | 17.3 | 7 | 24.1 | 1,451 | 19.3 | ||
| Age | ||||||||||||
| <29 years | 1,515 | 24.4 | 229 | 21.1 | 41 | 20.3 | 4 | 13.8 | 1,789 | 24.0 | ||
| 30-49 years | 3,023 | 48.8 | 571 | 52.6 | 102 | 50.5 | 13 | 44.8 | 3,709 | 49.3 | ||
| >50 years | 1,660 | 26.7 | 285 | 26.3 | 59 | 29.2 | 12 | 41.4 | 1,345 | 26.7 | ||
| Unknown | 3 | 0.1 | 0 | 0 | 0 | 0 | 0 | 0 | 3 | 0 | ||
| Exposure | ||||||||||||
| Occupational | 2,413 | 38.9 | 692 | 63.8 | 104 | 51.5 | 10 | 34.5 | 3,219 | 42.8 | ||
| Non-Occupational | 903 | 14.6 | 212 | 19.5 | 68 | 33.7 | 14 | 48.3 | 1,197 | 15.9 | ||
| Both | 1513 | 2.4 | 45 | 4.2 | 14 | 6.9 | 3 | 10.3 | 213 | 2.8 | ||
| Unknown | 2,734 | 44.1 | 136 | 12.5 | 16 | 7.9 | 2 | 6.9 | 2,888 | 38.4 | ||
| Geographic Area | ||||||||||||
| NYS w/o NYC | 3,247 | 52.4 | 580 | 53.5 | 111 | 55.0 | 18 | 62.1 | 3,956 | 52.6 | ||
| NYC | 2,323 | 37.5 | 377 | 34.8 | 71 | 35.2 | 11 | 37.9 | 2,782 | 37.0 | ||
| Out of NY | 566 | 9.1 | 116 | 10.7 | 18 | 8.9 | 0 | 0 | 700 | 9.3 | ||
| Unknown | 65 | 1.0 | 12 | 1.0 | 2 | 1.0 | 0 | 0 | 79 | 1.1 | ||
| * Note: Due to rounding, some percentage columns may not sum to 100. | ||||||||||||
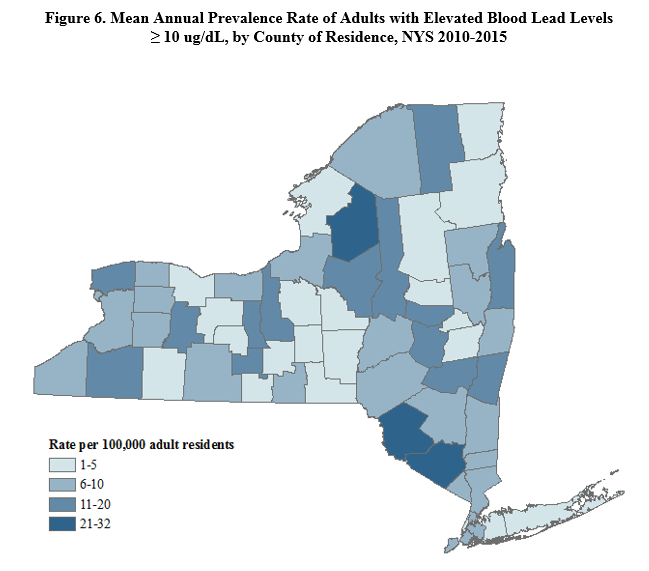
The county of residence for individuals reported with elevated blood lead levels (greater than or equal to 10 µg/dL) is displayed in Figure 6. While this figure shows where people who get tested live, there is no obvious pattern in the geographic distribution of the individuals. There are a number of people who reside out of state (Table 5), but are exposed to lead due to work in NYS.
Figure 6. Distribution of Tested Adults Reported with Peak Blood Lead Levels ≥10 ug/dL, by County of Residence, 2006-2010
As used in this report, the term occupational includes exposures that are classified as occupational exposures only, or both occupational and non-occupational. The primary sources of lead for occupationally exposed individuals with elevated blood lead levels (greater than or equal to 10 µg/dL) are displayed in Table 6. Individuals included in the "other" category had occupational exposures that were not included in any of the categories described in Table 6. These people were primarily machine operators, assemblers and non-construction laborers working in the manufacture of primary metals, electronics and electrical.
| Exposure Source | Blood Lead Levels (µg/dL) | ||||
|---|---|---|---|---|---|
| 10-24 | 25-39 | 40-59 | >60 | Total | |
| Bridge Work | 543 | 265 | 29 | 0 | 837 |
| Iron/Steel Structures | 150 | 53 | 14 | 1 | 218 |
| Target Shooting | 119 | 27 | 7 | 1 | 154 |
| Residential Remodeling | 70 | 33 | 9 | 5 | 117 |
| Lead Abatement | 78 | 15 | 4 | 1 | 98 |
| Cables/Wire Work | 77 | 12 | 3 | 0 | 92 |
| Metal Recycling | 70 | 13 | 4 | 0 | 87 |
| Foundry/Smelting | 55 | 16 | 2 | 0 | 73 |
| Stained Glass | 33 | 17 | 0 | 0 | 50 |
| Lead Glass/Powder | 11 | 3 | 0 | 0 | 14 |
| Radiator Repair | 7 | 0 | 2 | 0 | 9 |
| Other | 1,414 | 290 | 44 | 5 | 1,753 |
| Unknown | 6 | 0 | 0 | 0 | 6 |
| Total | 2,633 | 744 | 118 | 13 | 3,508 |
The primary sources of non-occupational exposure among individuals with blood lead levels greater than or equal to 10 µg/dL are displayed in Table 7. Individuals with non-occupational exposures are primarily exposed through the use of folk medicines/dietary supplements, during target shooting and during residential remodeling. Lead has been found in some traditional folk medicines used by South Asian, Middle Eastern and Hispanic cultures. In some cultures, people believe that lead can be useful in treating ailments such as arthritis, infertility, and upset stomach.8 These exposures primarily occur in the NYC area, and the NYC Department of Health and Mental Hygiene has developed many outreach materials to address these exposures.9 Exposure to lead is also a concern during the renovation/remodeling of any home built before 1978, after which lead was banned from household paint. NYSDOH has developed outreach materials and staff routinely assists homeowners in assessing and reducing their potential for exposure. People can also be exposed to lead from target shooting since most ammunition contains lead in either the bullet or the primer. Details about an industrial hygiene evaluation of two shooting ranges, are presented elsewhere in this report. The highest non-occupational blood lead levels (over 60 µg/dL) occurred among those using folk medicines/dietary supplements, target shooters, and residental remodelers.
| Exposure Source | Blood Lead Levels (µg/dL) | ||||
|---|---|---|---|---|---|
| 10-24 | 25-39 | 40-59 | >60 | Total | |
| Folk Remedies | 302 | 47 | 19 | 6 | 374 |
| Target Shooting | 230 | 93 | 23 | 3 | 349 |
| Residential Remodeling | 116 | 35 | 12 | 3 | 166 |
| Household Environment/Home Product* | 72 | 6 | 1 | 1 | 80 |
| Retained Bullet Fragments** | 31 | 13 | 5 | 0 | 49 |
| Pica | 21 | 8 | 5 | 0 | 29 |
| Cookware | 27 | 2 | 0 | 0 | 29 |
| Casting of Bullets, Fish Sinkers | 13 | 2 | 5 | 1 | 21 |
| Hobby, Jewelry, Crafts | 8 | 2 | 0 | 0 | 10 |
| Unknown | 266 | 51 | 12 | 3 | 332 |
| Total | 1,086 | 259 | 82 | 17 | 1,444 |
|
|||||
Adult Blood Lead Epidemiology and Surveillance
NYS participates in the National Institute for Occupational Safety and Health (NIOSH) surveillance program, Adult Blood Lead Epidemiology and Surveillance (ABLES), which is a state-based surveillance program of laboratory-reported adult blood lead levels.10 For the ABLES program, adults are defined as persons 16 years or older. The objective of the ABLES program is to build state capacity to improve adult blood lead surveillance programs and to measure trends in adult blood lead levels. NYSDOH submits lead data from the HMR to the ABLES program annually Nationally, 41 states participate in ABLES. OSHA has used national program data to identify industries where elevated blood lead levels indicate a need for national focus. Over the past 17 years, a 50 percent decrease in the national prevalence rates of blood lead levels 25 µg/dL or greater has been documented using ABLES data. NYSDOH has used ABLES data to identify trends and identify areas for targeted interventions.
Disparities in Lead Exposure
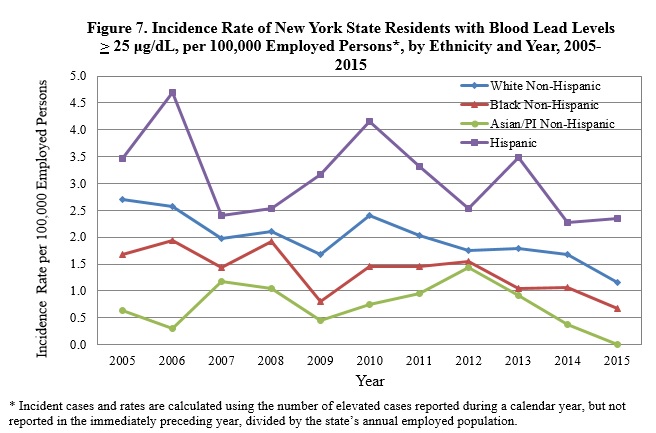
As shown in Figure 7, there has generally been a decline in the incidence rate of elevated adult blood lead levels (25 µg/dL or greater) among various groups of New Yorkers during the time period 2010-2015. However, Hispanics still have almost double the rate of elevated blood lead levels compared to other groups.
Hispanic females made up almost 40 percent of all females with a known ethnicity reported to the HMR with blood lead levels 25 µg/dL or greater between 2005 and 2015. More than 80 percent of these Hispanic women had non-occupational exposure due to folk remedy use, and approximately 90 percent resided in NYC. Most of the Hispanic men reported to the HMR, 57 percent of whom reside in the NYC area, were exposed to lead through their jobs as bridge workers (data not shown). The data show the continuing need for educational outreach to Hispanic women and men.
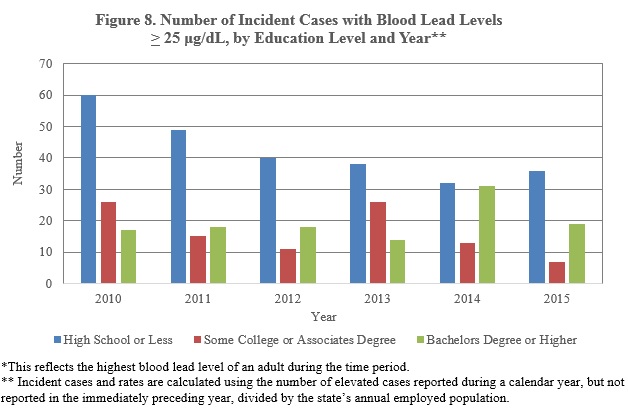
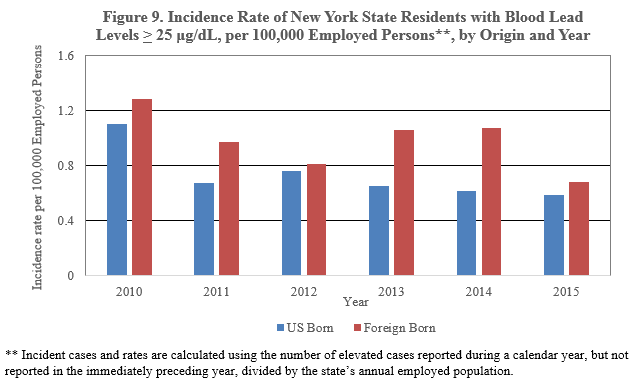
The large majority of workers with incident blood lead levels 25 µg/dL or greater during 2010-2015 had a high school diploma or less (Figure 8). Workers with up to a high school education were mostly exposed to lead through working in construction, while workers with bachelor’s degrees or higher were exposed to lead through recreational residential remodeling and target shooting (data not shown). Foreign-born workers comprised approximately 30 percent of workers with blood lead levels of 25 µg/dL or greater and their primary lead exposure source was bridge construction, non-bridge construction and folk medicine use. The incidence rate of blood lead levels of 25 μg/dL or greater for foreign-born workers was higher than the rate for US born workers (Figure 9).
Mercury
Mercury occurs naturally in the environment in several forms. One common form is metallic mercury (also called elemental mercury). Metallic mercury is a silvery, odorless liquid that can evaporate at room temperature, becoming a vapor. Mercury can also combine with other chemicals to form inorganic or organic mercury compounds. Inorganic mercury is mercury combined with other chemical elements such as chlorine, sulfur or oxygen. Organic mercury is mercury combined with carbon-based compounds. One common form of organic mercury is methylmercury, which is produced by microorganisms in water and soil, and accumulates in fish. Exposure to high levels of mercury can damage the nervous system and cause irritability, shyness, tremors, changes in vision or hearing and memory problems. Mercury can also harm the kidneys and developing fetus.11 People are exposed to metallic mercury when they inhale the vapors. People can be exposed to inorganic and organic mercury when they eat foods or other products contaminated with mercury.
Urine and blood testing are the accepted methods to assess mercury exposure for medical purposes. The type of test performed depends upon the form of mercury to which a person may have been exposed. An elevated urine test for mercury indicates an elemental or inorganic source of mercury exposure. An elevated blood test for mercury indicates a recent exposure to a high concentration of mercury vapor or exposure to an organic mercury source (for example, methylmercury from a recent fish meal). Levels of mercury that are reportable to the NYSDOH are 5 ng/mL in blood and 20 ng/mL in urine.
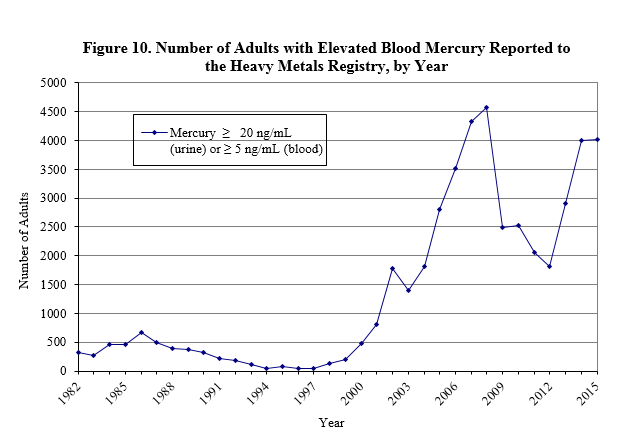
The number of adults with elevated blood mercury reported to the HMR began to sharply increase in 2000, peaking at 4,575 adults reported in 2008 (Figure 10). Between 2010 and 2015, 13,596 adults were tested for mercury. Because some individuals were tested more than once, there were a total of 19,997 tests during this period (Table 8). These individuals were almost equally divided between males (48.9%) and females (50.9%), and more than half were 50 years of age and older. Almost 60 percent of those tested were residents of NYC.
Approximately 99% of adults reported to the HMR, with an identifiable exposure source, had non-occupational exposures resulting from seafood consumption. Commonly consumed fish included salmon, tuna, and swordfish, with more than 90% of adults eating seafood a few times or more per week.
| Number of Adults | N | % |
|---|---|---|
| 13,596 | ||
| Sex | ||
| Male | 6,651 | 48.9 |
| Female | 6,921 | 50.9 |
| Age | ||
| <29 years | 1,1443 | 8.4 |
| 30-49 years | 4,721 | 34.7 |
| >50 years | 7,731 | 56.9 |
| Exposure | ||
| Occupational | 21 | 0.2 |
| Non-Occupational | 1,318 | 9.7 |
| Both | 4 | 0.0 |
| Unknown | 12,253 | 90.1 |
| Geographic Area | ||
| NYS w/o NYC | 4,780 | 35.2 |
| NYC | 7,681 | 56.5 |
| Out of State/Unknown | 1,135 | 8.3 |
| Total Number of Tests* | 19,997 | |
| * The number of tests adds up to more than the number of adults because many adults have multiple mercury tests. | ||
HMR Research and Intervention Activities
NYSDOH continually reviews and evaluates data from this Registry and uses this information to design and implement prevention efforts. For example, data from the HMR have proven to be an important tool in research to identify situations in which adult lead exposure is occurring and the consequences of the exposures. Some examples are listed below.
Identifying Causes of Elevated Blood Lead Levels
- An in-depth 10-year analysis of lead exposures among NYS adults showed that the types of lead exposure vary by gender, race and ethnicity. For example, women are primarily exposed to lead via non-occupational activities, while the primary source of exposure for men is occupational. The analysis also examined trends in time over the 10-year period. The details of the analysis have been made available on the NYSDOH Occupational Health Surveillance page.
- The NYSDOH continues to participate in the National Institute for Occupational Safety and Health (NIOSH) surveillance program, Adult Blood Lead Epidemiology and Surveillance Programs (ABLES), which is a state-based surveillance program of laboratory-reported adult blood lead levels. The objective of the ABLES program is to build state capacity to improve and enhance adult blood lead surveillance programs and to measure trends in adult blood lead levels. NYSDOH submits lead data from the HMR to the ABLES program annually. Over the last 18 years, a 54% decrease in the national prevalence rates of blood lead levels 25 µg/dL has been documented using ABLES surveillance data. ABLES data, including data from the HMR, has been used to illustrate the persistent problem of adults with very high blood lead levels in the United States.
Actions to Help Reduce Blood Lead Levels
- HMR staff worked with staff from the Center for Environmental Health’s Outreach and Education (O&E) unit to redesign the brochure: Health Dangers from Lead on the Job. The brochure is designed to provide educational information regarding the hazards of working with lead and is mailed to NYS workers or residents who are reported to the HMR with blood lead levels greater than or equal to 10 µg/dL. Recommendations found in the brochure were updated to better reflect the latest scientific studies regarding the toxicity concerns of low-level lead doses in adults. Emphasis was placed on ensuring the brochure was appropriate for lower literacy groups. Worker focus groups were used to evaluate the revisions, and subsequent changes to the brochure were made using the input of the focus groups
- Industrial hygiene staff continues to conduct outreach and provide educational materials, including the NYSDOH fact sheet Aim at Lead Safety, to both residents and workers, regarding lead exposure in firing ranges. Ongoing technical guidance is provided to employers requesting assistance on methods to reduce exposure to lead.
Lead Exposed Pregnant Women and Follow-Up Testing of Their Newborns
- 1 New York State Department of Health Heavy Metals Surveillance. Arsenic. Available at: http://www.health.ny.gov/environmental/workplace/heavy_metals_registry/arsenic.htm. Accessed June 2016.
- 2 Agency for Toxic Substances and Disease Registry, 2007. Toxicological Profile for Arsenic (Update). Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service.
- 3 New York State Department of Health Heavy Metals Surveillance. Cadmium. Available at:http://www.health.ny.gov/environmental/workplace/heavy_metals_registry/cadmium.htm. Accessed June 2016.
- 4 Agency for Toxic Substances and Disease Registry. 2012. Toxicological Profile for Cadmium. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service.
- 5 Agency for Toxic Substances and Disease Registry. 2007. Toxicological Profile for Lead (Update). Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service.
- 7 New York State Department of Health, American College of Obstetricians and Gynecologists, District II. Lead poisoning prevention guidelines for prenatal care providers. Albany (NY): New York State Department of Health; June 2009. Available at: http://www.health.ny.gov/publications/2535.pdf. Accessed June 2016.
- 8 Centers for Disease Control and Prevention. National Center for Environmental Health. Folk Medicine. http://www.cdc.gov/nceh/lead/tips/folkmedicine.htm . Updated June 2013. Accessed June 2016.
- 9 New York City Department of Health and Mental Hygiene. Remedies or Herbal Medicines Containing Lead. Available at: https://www1.nyc.gov/site/doh/health/health-topics/lead-poisoning-contaminated-herbal-medicine-products.page?_sm_au_=iVV4DR6VPbPVP7J6 Accessed June 2016.
- 10Alarcon, WA. Elevated Blood Lead Levels Among Employed Adults – United States, 1994-2013. 63(55):Morbidity and Mortality Weekly Report, 2016.
- 11 Agency for Toxic Substances and Disease Registry. 1999. Toxicological Profile for Mercury. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service.
- 12 Bellinger DC. Teratogen update: lead and pregnancy. Birth Defects Res A Clin Mol Teratol 2005; 73:409-20.
- 13 Lin S, Hwang SA, Marshall EG, Marion D. Does Paternal Occupational Lead Exposure Increase the Risks of Low Birth Weight or Prematurity? Am J Epidemiol 1998; 148:173-181
- 14 Bellinger DC, Hu H, Kalaniti K. et al. A pilot study of blood lead levels and neurobehavioral function in children living in Chennai, India. Int J Occup Environ Health. 2005;11(2):138–143.
- 15Riess ML, Halm JK. Lead poisoning in an adult: Lead mobilization by pregnancy? J Gen Intern Med2007; 22: 1212–1215.
- 17Centers for Disease Control and Prevention. Guidelines for the identification and management of lead exposure in pregnant and lactating women. Atlanta (GA): CDC; 2010. Available at: http://www.cdc.gov/nceh/lead/publications/leadandpregnancy2010.pdf. Updated November 2010. Accessed November 2016.
Lead poisoning is an important concern for both pregnant women and women of preconception age. Prenatal lead exposure has known adverse effects on maternal health and infant outcomes across a wide range of maternal lead levels.12 Adverse effects of lead exposure are also being identified at lower levels of exposure than previously recognized in both children and adults. A pregnant woman with an elevated blood lead level may experience maternal hypertension, preterm delivery, miscarriage or stillbirth. Maternal lead can readily cross the placenta and enter the fetus’ blood circulation, making the fetus susceptible to lead poisoning.13 Studies have shown that children born to mothers with elevated blood lead levels are at increased risk for having elevated blood lead levels at birth and associated cognitive and developmental delays.14 Data from the HMR show that women of childbearing age may be exposed to lead during pregnancy from home renovation and repairs, occupational exposures, or other sources such as imported pottery, spices, foods, cosmetics and health remedies from other countries (e.g., herbs and Ayurvedic medicines). During pregnancy, maternal lead may be mobilized from bone stores into the bloodstream and then cross the placenta or enter the breast milk.15
Although NYS law does not require testing all pregnant women for blood lead, regulations state that a health care provider should test those pregnant women at high risk, and the state has established guidelines for health care practitioners to assist them in determining a woman’s risk of lead poisoning on her initial prenatal visit.7 Women of childbearing age (16-45) with blood lead levels of 10 µg/dL or higher are routinely interviewed by HMR staff to determine the possible sources of exposure, to provide advice on appropriate control measures to limit future exposures and to answer questions. In the interview, information is collected on whether anyone in the home is pregnant or nursing, and if pregnant, the expected due date. If during the course of the interview, a woman is identified as pregnant, information is also obtained on her expected due date and the name and contact information of her physician, if she has one. HMR staff will contact the woman’s physician to collect additional information on the patient but also to share information obtained during the interview regarding the potential source of lead exposure, to remind the physician to continue to test the woman for lead throughout their pregnancy, and to provide any additional resources, as requested. The woman is also mailed an informational brochure on ways to reduce her exposure and how to minimize or eliminate future lead exposures.
HMR staff also subsequently contacts the local health department to share the information about the pregnant women with them. The local health department will discuss their plan for follow-up with HMR staff. If the local health department intends to go to the pregnant woman’s home for inspection, or has been there in the past, this information is shared with HMR staff. State health department staff work with the county to identify the pediatrician. HMR staff will call the woman’s obstetrician to remind them to share all blood lead level information with the pediatrician and will also confirm the pediatrician. HMR staff also collaborates with the childhood lead program and has access to the childhood lead database, so they are able to see if/when the newborn baby is tested for lead, and what the child’s level is. Prior to the birth of the infant, HMR staff will also confirm the pediatrician is aware of the maternal blood lead level. Follow-up with all necessary parties will occur until the newborn is tested for lead.
The follow-up of pregnant women and their newborn babies has been ongoing since 2013. Since that time, a total of 127 pregnant women with elevated blood lead levels have been identified. Thirty-three percent are first pregnancies, while 67% are subsequent pregnancies. Some exposures among this population include spice consumption, residential, Ayurveda, pica/lodged bullet, cosmetics, and occupational, and many women have multiple sources of lead exposure (Table 9). It is important to note, that the use of spices, many of them brought in from outside the country, have increased in usage among this population. In addition, when accounting for multiple sources of exposure, spices made up approximately 47% of all exposure sources in 2015, which is an increase from 17% in 2013.
| Sources of Exposure | 2013 (52 cases) | 2014 (32 cases) | 2015 (43 cases) |
|---|---|---|---|
| Unknown | 34.6% | 34.0% | 28.0% |
| Spices Only | 5.6% | 9.0% | 28.0% |
| Residential | 11.5% | 13.0% | 14.0% |
| Country Burden | 7.6% | 0% | 2.0% |
| Imported Candy Only | 7.6% | 3.0% | 0% |
| Cookware/Pottery Use Only | 7.6% | 13.0% | 0% |
| PICA/Bullet/Cosmetics/Occupational(Potter) | 7.6% | 3.0% | 4.0% |
| Ayurveda Only | 2.0% | 0% | 4.0% |
| Multiple Sources (Spices + 1 Other) | 11.5% | 24.0% | 19.0% |
New York State Public Health Law and Regulations require health care providers to obtain a blood lead test for all children at age one and again at age two. In 2013, 78% of all babies born to a pregnant mother with an elevated blood lead test were tested for lead prior to turning one. This percentage increased to 100% in both 2014 and 2015, which is consistent with the Centers for Disease Control and Prevention (CDC’s) recommendation for follow-up blood lead testing for all newborn infants born to mothers with blood lead levels equal to and greater than 5 µg/dL. It is also important to note that the average ‘initial’ blood lead level of the pregnant mother has decreased from 15.6 µg/dL in 2013 to 14.2 µg/dL in 2015 (Table 10).
| 2013 (52 cases) | 2014 (32 cases) | 2015 (43 cases) | |
|---|---|---|---|
| % of lead tests conducted for newborn as a result of BOHIP/county outreach | 78% | 100% | 100% |
| Average ‘initial BLL (µg/dL) of pregnant woman | 15.6 | 15.2 | 14.2 |
The collaboration between HMR staff and county health departments are providing the all-important link between pediatric providers and obstetric practice to ensure that no baby born to a mother with an elevated blood lead level falls through the lead testing crack.
References
Appendix A: State Regulations for Reporting Heavy Metals
22.6 Reporting heavy metals in blood and urine. Every physician, clinical laboratory and health facility in attendance of a person with a blood or urine test resulting in a value at or above those listed in section 22.7 of this Part, shall report such occurrence to the State Commissioner of Health within 10 days of the receipt of the results of such test. The report shall be on such forms as prescribed by the State Commissioner of Health.
Historical Note: Sec filed May 14, 1981 eff. Dec. 1, 1981.
22.7 Reportable levels of heavy metals in blood and urine. For purposes of section 22.6 of this Part, the following levels of heavy metals in blood and urine samples are reportable to the State Commissioner of Health:
| Metal | Sample | Reportable At or Above |
|---|---|---|
| Lead | Blood | All levels |
| Cadmium | Blood | 10 nanograms per milliliter |
| Urine | 5 micrograms per liter | |
| Mercury | Blood | 5 nanograms per milliliter |
| Urine | 20 nanograms per milliliter | |
| Arsenic | Urine | 50 micrograms per liter |
Historical Note: Sec filed May 14, 1981, and filed Sept. 11, 1986, eff. Sept. 11, 1986
Subpart 67-3
REPORTING OF BLOOD LEAD LEVELS
SEC 67-3.1 Laboratory reporting of blood lead levels for public health follow up
Section 67-3.1 Laboratory reporting of blood lead levels for public health follow up.
(a) For purposes of this Subpart, laboratory shall mean any laboratory that holds a permit issued in accordance with Public Health Law Article 5, Title V and is authorized to conduct blood lead analyses.
(b) Laboratories shall report the results of all blood lead analyses performed on residents of New York State to the Commissioner of Health and to the local health officers in whose jurisdictions the subjects of the tests reside. If the laboratory reports electronically to the Commissioner of Health in accordance with subdivision (e) below, the Department of Health shall notify the appropriate local health officer of the test results and the laboratory shall be deemed to have satisfied the reporting requirements of this section.
Appendix B: Overview of Heavy Metals Registry Program Operations
Clinical laboratories, physicians and health care facilities can report heavy metal test results electronically through the internet or manually on paper forms to the DOH. All information reported to the Registry is confidential, and records and computer files are maintained in accordance with DOH regulations concerning medical data containing individual identifiers. Access to the data by anyone other than Registry personnel is restricted and carefully monitored so that confidentiality is maintained. Approximately 99% of all tests for lead were submitted electronically. This was similar for tests of other heavy metals: 95% of arsenic, 75% of mercury, and 100% of cadmium tests were all submitted electronically.
Once information is received on a person with an elevated level, DOH contacts the person and/or their physician and interviews them to determine the possible sources of exposure, provide advice on appropriate control measures to limit future exposures to the individual and his or her family, and answer any questions the individual may have. DOH also collects demographic information, such as level of education, primary language spoken, and ethnicity along with information about the subject's work and home environments. When the exposure is work-related, DOH gathers information on the employer, work location, protection measures in place and whether coworkers are also potentially exposed. When the exposure is work-related, DOH gathers information on the employer, work location, protection measures in place and whether coworkers are also potentially exposed. Following the interview, DOH provides individuals with brochures appropriate to their exposure sources describing methods to reduce exposure, along with the telephone number of the local state-sponsored occupational health clinic in the event they wish to pursue additional follow-up on their test results (a list of NYS Occupational Health Clinic locations and contact information can be found at: https://www.health.ny.gov/environmental/workplace/clinic.htm.
DOH performs the contacts described above for all individuals with reportable levels of arsenic and cadmium, or reportable urine mercury level. For mercury in blood, many years of experience have shown that lower levels of blood mercury are almost always due to eating freshwater fish and seafood.18 Therefore, effective February 2014, only those individuals with blood mercury levels at or above 60 ng/mL are interviewed. A fact sheet about potential sources of mercury exposure and prevention techniques is mailed to all others not interviewed. Prior to that, interviews occurred at or above blood mercury levels of 25 ng/mL. Currently, interviews are conducted for lead exposures of women of childbearing age (ages 16-45), and 16 and 17 year olds with blood lead levels greater than or equal to 10 µg/dL. For all other adults, the interviews are conducted for anyone with blood lead levels at or above 15 µg/dL. All children are followed by the NYSDOH Childhood Lead Poisoning Primary Prevention Program. DOH regularly sends letters advising pregnant women to have their newborns tested at birth and works directly with the local health departments on case management.
When DOH identifies a workplace with employees with high or persistently elevated heavy metal levels, DOH conducts follow-up with the employer. For situations where an employer has not previously had an employee who was reported to the HMR, an industrial hygienist contacts the company to determine the exposure circumstances, learn whether coworkers are at risk and assess whether the company is taking appropriate measures to control exposures. With all contacts, the industrial hygienist protects the confidentiality of the individual reported. An important focus of these efforts is smaller businesses that do not have either full-time medical or industrial hygiene resources to evaluate their worksites. At a minimum, DOH provides advice over the telephone, with a follow-up letter summarizing the recommendations. Depending on the severity or persistence of the problem, or the uniqueness of the source of exposure, DOH may ask for permission to conduct an on-site industrial hygiene evaluation. That evaluation is then followed by a written report that is submitted to the employer and to the union representative, if applicable. .
In all cases, DOH's goal is to reduce exposure to all heavy metals. For workplace exposures, DOH recommendations are guided by the federal Occupational Safety and Health Administration (OSHA) standards and the experience of the industrial hygienists in addressing similar exposures. In these instances, DOH encourages employers to implement site-specific exposure reduction measures and monitoring to help assure that exposures have been reduced.
The HMR database is an interactive system which is updated daily. Both blood lead and other heavy metal reports are received electronically from laboratories daily, and are added to the database each morning. All surveillance and follow-up information is available to DOH instantly as changes and updates occur. This greatly enhances the ability of DOH to determine if a report has already been received; correct report and case data immediately; make new information directly available to all staff; uncover and correct errors, add new employers, assign cases to interviewers and track the progress of cases with elevated test results, daily. Daily updates allow staff to rapidly respond to highly elevated levels to ensure that the case is receiving proper medical management, to identify others at risk, and to intervene to prevent further exposures.
