Conference of Local Mental Hygiene Directors
- Slides also available in Portable Document Format (PDF)

Overview of Design of Health Home Model for Children
Conference of Local Mental Hygiene Directors
NYS Department of Health
April 6, 2015
Agenda
- Today: Overview and Update of Key Design Elements of Health Home and Transition of Behavioral Health Benefit to Managed Care
- April 29, 2015: More Detailed Update on the Development of Design Elements for Health Home Model for Children
Key Medicaid Redesign Team Initiatives for Improving and Integrating Health Care Services for Children
- Enrollment of Children in Health Homes: October 2015
- Transition of Behavioral Health and Foster Care populations into Managed Care: January 2016
- Both initiatives work together to provide care management to children, integrate the delivery of physical and behavioral health services, identify and address needs early to prevent escalation and longer term need for higher end services, maintain child in community and at home with support services
- Today´s discussion overview of Health Home for Children Key Design Elements how Health Home for Children is integrated into design of Behavioral Health transition
| Anticipated Schedule of Activities for Expanding Health Homes to Better Serve Children | Due Date |
|---|---|
| Draft Health Home Application to Serve Children Release | June 30, 2014 –Completed |
| Due Date to Submit Comments on Draft Health Home Application to Serve Children | July 30, 2014 –Completed |
| Due Date to Submit Letter of Interest | July 30, 2014 –Completed |
| Final Health Home Application to Serve Children Released | November 3, 2014 –Completed |
| Due Date to Submit Health Home Application to Serve Children | March 2, 2015 –Completed |
| Review and Approval of Health Home Applications to Serve Children by the State | March 2, 2015 to June 15, 2015 Review Process Underway |
| HH and Network Partner Readiness Activities | June 15, 2015 to September 30,2015 |
| State Webinars, Training and Other Readiness Activities | Through September 30, 2015 |
| Begin Phasing–in the Enrollment of Children in Health Homes | October 2015 |
| Children´s Behavioral Health Services and other Children´s Populations Transition to Managed Care | January 2016 |
Engaging Stakeholders in the Design of the Health Home Model for Children
- On June 30, 2014 the State issued a draft design document, that included a draft Health Home Application to Serve Children, and sought stakeholder feedback on key areas of the design, including:
- Eligibility requirements
- Requirements for expanding Health Home networks to reflect the needs of children
- Requirements for demonstrating Health Homes can "tailor" delivery of core Health Home services to better serve children
- Connectivity with programs and systems that impact children (foster care, education, Early Intervention)
- Stakeholder Comments were due July 30, 2014
- Applications were due March 2, 2015
- Review process by Multi–Agency Team now underway
- Design discussions with continue, next discussion April 29, 2015
Tailoring Health Homes to Serve Children and Transition of Behavioral Health Benefit for Children to Managed Care ~ A Collaborative Effort of State Agency Partners and Stakeholders
- State Agency Partners
- Office of Mental Health (OMH)
- Office of Alcoholism and Substance Abuse Services (OASAS)
- Office of Children and Family Services (OCFS)
- Department of Health (DOH) (including Office of Health Insurance Programs, Center for Health–Division of Family Health, AIDS Institute)
- New York State Education Department
- Stakeholders
- Health Homes, Managed Care Plans and Care Managers
- Associations
- Advocates
- Local Government Partners (LDSS, CLMHD, LGU, SPOA, NYCDOHMH)
Principles for Serving Children in Health Homes and Managed Care
- Ensure managed care and care coordination networks provide comprehensive, integrated physical and behavioral health care that recognizes the unique needs of children and their families
- Provide care coordination and planning that is family–and–youth driven, supports a system of care that builds upon the strengths of the child and family
- Ensure managed care staff and systems care coordinators are trained in working with families and children with unique, complex health needs
- Ensure continuity of care and comprehensive transitional care from service to service (education, foster care, juvenile justice, child to adult)
- Incorporate a child/family specific assent/consent process that recognizes the legal right of a child to seek specific care without parental/guardian consent
- Track clinical and functional outcomes using standardized pediatric tools that are validated for the screening and assessing of children
- Adopt child–specific and nationally recognized measures to monitor quality and outcomes
- Ensure smooth transition from current care management models to Health Home, including transition plan for care management payments
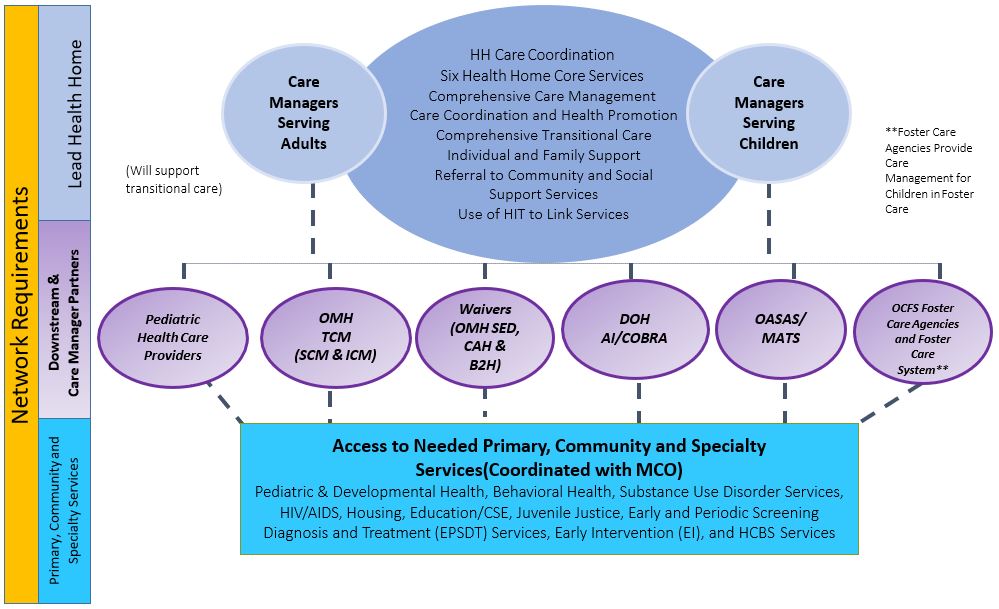
New York State Health Home Model for Children
Managed Care Organizations (MCOs)
Health Home
Administrative Services, Network Management, HIT Support/Data Exchange
Enacted Budget
- Includes $45 million in 2015–16 and $90 million in 2016–17 for the enrollment of children in Health Homes (i.e., PMPM costs)
- Includes technical amendment to provide a total of $20 million in Managed Care (MC) and Health Home Readiness resources for Foster Care agencies
- Both are in addition to other MC Readiness available for children
Design Elements:
Expanding Health Home Eligibility Criteria for Children
- Current Eligibility Criteria is condition–based (per Affordable Care Act (ACA)):
- At least 2 chronic conditions (e.g., substance abuse disorder, diabetes, asthma, heart disease, over weight (BMI> 25), hypertension, or
- Serious Mental Illness, or
- HIV/AIDS
- Must be "appropriate" for Health Homes
- Goal: Consistent with Stakeholder feedback, modify Health Home eligibility condition–based criteria (as required by ACA) that captures the following children´s populations:
- Medically fragile children with complex health issues, children in foster care, children with SED, children enrolled in current Waiver programs and other case management programs
- No changes to current eligibility criteria required to capture children with:
- Serious Emotional Disturbance (SED)
- ✓ Serious Mental Illness (currently a single qualifying condition for HHs) is interpreted under the ACA to include SED
- ✓ SED will be single qualifying condition for Health Home
- Serious Emotional Disturbance (SED)
- Medically Complex Conditions (Medically Fragile Children)
- ✓ Based on information submitted by Stakeholders and discussions with clinicians, the State believes that most Medically Fragile Children with complex medical conditions that would need the intensive care management provided by a HH will have at least two chronic conditions
- Children and adolescents with HIV
Design Elements – Definition of SED for Health Home Eligibility
- Goal in developing the SED definition for Health Home eligibility was to be consistent with the OMH SED definition, which relies upon the Diagnostic and Statistical Manual of Mental Disorders (DSM), and the chronic condition eligibility requirements of the Health Home Program.
- Serious Emotional Disturbance (SED): A child or adolescent (under the age of 21) that has a designated mental illness diagnosis as defined by the most recent version of the DSM AND has experienced functional limitations due to emotional disturbance over the past 12 months (from the date of assessment) on a continuous or intermittent basis.
- The State is finalizing work to finalize SED definition for Health Home – April 29, 2015 Webinar
- It is expected that that SED definition for Health Home will include diagnoses at least from the following DSM–5 categories: Bipolar and Related Disorders; Depressive Disorders; Feeding and Eating Disorders; Schizophrenia Spectrum and Other Psychotic Disorders; Obsessive– Compulsive Related Disorder; Disruptive, Impulse Control and Conduct Disorders; and Personality Disorders
- To meet the SED criteria functional limitations must exist in the following areas (unchanged from Draft Application)
- Ability to care for self (e.g. personal hygiene; obtaining and eating food; dressing; avoiding injuries); or
- Family life (e.g. capacity to live in a family or family like environment; relationships with parents or substitute parents, siblings and other relatives; behavior in family setting); or
- Social relationships (e.g. establishing and maintaining friendships; interpersonal interactions with peers, neighbors and other adults; social skills; compliance with social norms; play and appropriate use of leisure time); or
- Self–direction/self–control (e.g. ability to sustain focused attention for a long enough period of time to permit completion of age–appropriate tasks; behavioral self–control; appropriate judgment and value systems; decision–making ability); or
- Ability to learn (e.g. school achievement and attendance; receptive and expressive language; relationships with teachers; behavior in school).
- In addition to clinical assessments, the Child Adolescent Needs and Strengths–NY (CANS) is being modified to help verify functional limitations
Design Elements:
Expanding Health Home Eligibility Criteria for Children
- Pending Centers for Medicare and Medicaid Services (CMS) approval, eligibility criteria for children would be expanded to include trauma and at risk for another chronic condition
- Definition of Trauma: Exposure to a single severely distressing event, or multiple or chronic or prolonged traumatic events as a child or adolescent, which is often invasive and interpersonal in nature. Trauma includes complex trauma exposure which involves the simultaneous or sequential occurrence of child maltreatment, including psychological maltreatment, neglect, exposure to violence and physical and sexual abuse.
- A child or adolescent who has experienced trauma would be defined to be at risk for another chronic condition if they have one or more functional limitations that interferes with their ability to function in family, school, or community activities, or they have been placed outside the home.
- ✓ Functional limitations are defined as difficulties that substantially interfere with or limit the child in achieving or maintaining developmentally appropriate social, behavioral, cognitive, communicative, or adaptive skills, or for a child who experienced trauma due to child maltreatment, a functional limitation is defined as a serious disruption in family relationships necessary for normal childhood growth and development.
- The Final Application includes a proposal to amend the Body Mass Index (BMI) > 25 to make the definition comparable to the Centers for Disease Control and Prevention (CDC) definition for overweight and to provide a comparable overweight measure for children as follows:
- Change "BMI > 25" to "BMI at or above 25 for Adults"
- Add "At or above the 85th percentile for children of the same sex and age"
- Children and adults that meet this revised overweight definition AND have one other chronic condition would be eligible for Health Home
Design Elements: Tailoring Appropriateness Criteria for Health Homes
- In addition to meeting the chronic condition criteria for Health Home (i.e., SED, Trauma and At Risk for Another Condition, HIV, at least two chronic conditions) members must be "appropriate" for Health Home, i.e., they need the more intensive level of care management provided by Health Homes
- In response to stakeholder comments the appropriateness criteria for Health Homes was amended (new changes are in green, and were reflected in Final Application)
- Appropriateness Criteria: Individuals meeting the Health Home eligibility criteria must be appropriate for Health Home care management. Assessing whether an individual is appropriate for Health Homes includes determining if the person is:
- At risk for an adverse event (e.g., death, disability, inpatient or nursing home admission, mandated preventive services, or out of home placement)
- Has inadequate social/family/housing support, or serious disruptions in family relationships;
- Has inadequate connectivity with healthcare system;
- Does not adhere to treatments or has difficulty managing medications;
- Has recently been released from incarceration, placement, detention, or psychiatric hospitalization;
- Has deficits in activities of daily living, learning or cognition issues, or
- Is concurrently eligible or enrolled, along with either their child or caregiver, in a Health Home.
Design Elements: Use of the Child and Adolescent Needs and Strengths Assessment of New York (CANS–NY)
- Stakeholders generally supported the use of the CANS–NY Assessment tool in the Health Home model
- CANS–NY is anticipated to be used:
- Determine need for Home Community Based Services
- Determine acuity for Health Home Rates
- Assist in determining if children meet HH eligibility functional criteria
- To address concerns the current CANS–NY tool may not adequately capture the various children´s populations that would be eligible for Health Home and HCBS services, including infants and toddlers and medically fragile children, the State is working to modify the CANS– NY to:
- Include modules specific to the 0–5 and 6–21 age groups
- Include a module related to sexuality and sexual orientation
- Include modules relating to Activities of Daily Living and Instruction on Activities of Daily Living to be in compliance with the Balancing Incentive Program;
- Make enhancements to better assess medically fragile children
- Modify the tool to determine functional limitations as provided by SED and Trauma HH eligibility criteria
- Develop an algorithm that will determine acuity tier (i.e., High, Medium, Low) for children´s Health Home rates
- The State has begun testing the modifications to the CANS–NY
- More detail on CANS tool and testing will be discussed on April 29, 2015
Design Elements: Health Home Per Member Per Month Rates for Children
- More detailed information on Health Home Per Member Per Month Rates anticipated to be discussed on April 29, 2015 Webinar
- Stakeholder comments focused on rate adequacy and low case load ratios
- The framework for the development of Per Member Per Month rates includes:
- Tiered rate structure (High, Medium, Low) based on acuity of child and the development of an algorithm using the modified CANS–NY
- Low care manger to child ratios that are preliminarily anticipated to range from 1:12 to 1:40 and for HFW (1:10)
- Lower case loads tied to higher acuity and higher rates; higher case loads tied to lower acuity and lower rates
- Flat rate for "outreach" activities
- Tiered rate structure would be in effect October 2015
- Tiered rate structure would be the mandated government rates in effect under the first two years of Managed Care (2016 and 2017)
- Legacy care management payments will be developed for children´s legacy providers (OMH TCM and B2H, CAH I/II, OMH Waiver Programs) and will remain in effect for two years
- Health Homes and managed care plans have the option of negotiating alternative payment arrangements if the Health Home, Plan and the State agree to such an alternative
Design Elements: Transitioning Existing Programs and Care Management Expertise to Health Homes
- OMH Targeted, Supportive and Blended Case Management Programs will convert to Health Homes in October 2015.
- Webinar for these programs/providers will be scheduled for shortly after the April 29, 2015 webinar
- Children´s 1915(c) Waiver Programs will begin to convert to Health Home January 2016 when the Behavioral Health Benefit transitions to Managed Care and
- OCFS Bridges to Health Programs (DD, MFC and SED)
- OMH Home and Community Based Services (HCBS) Program
- Care At Home (CAH) I and II
- Date is coincident with date behavioral health benefit and HCBS services are moved to Managed Care and such populations move to Managed Care
- State working on detailed plan to transition and phase–in children enrolled in Waiver Programs
- Waiver agencies and care managers are strongly encouraged to bring their care management expertise to Health Homes in 2015 by working now to join Health Home networks and to provide Health Home care management services to non–waiver children that will be enrolled in Health Homes beginning October 2015.
Design Elements: Children with Developmental Disabilities
- Children receiving services from the Office for People with Developmental Disabilities (OPWDD), including children in the Care at Home III, IV, and VI Waivers will not be prioritized at this time for enrollment into Health Home.
- However, DOH is continuing to work with OPWDD to discuss approaches for beginning to enroll children in Health Homes that have a developmental delay diagnosis and one other Health Home chronic condition or a single qualifying Health Home chronic condition and require the level of care management services provided by Health Home and who are not currently receiving OPWDD services that require OPWDD service coordination
High Fidelity Wraparound and Health Home
- Wraparound is a planning process that follows a series of prescribed steps to help children and their families realize a life that reflects their hopes and dreams.
- Focused on making sure children and youth grow up in their homes and communities.
- Brings people together from different parts of the family´s life with help from one or more facilitators, people from the family´s life work together, coordinate their activities, and move closer together in their view of the family´s situation.
- State is working on launching a HFW pilot to inform the incorporation of HFW within in Health Home – would be for the highest of the highest needs children – more details will be available on April 29, 2015 Webinar
Design Elements: Establishing Linkages with Children´s Systems of Care
- State is continuing to work with children´s systems of care to identify natural points in these systems where children can be identified and referred to Health Home (i.e., Medicaid Analytics Performance Portal (MAPP) Internet Referral Portal) and to provide Health Home "101"and Eligibility Training
- Education: State working with State Education Department
- Juvenile Justice: Initial discussions will cover juvenile probation, OCFS licensed detention programs, foster care agencies serving JDs, and OCFS facilities
- Local Government Units and Local Department of Social Services
- Providers
Design Elements: Foster Care and Health Homes
- Health Homes (HH) must contract with Voluntary Foster Care Agencies (VAs) to provide care management for children in foster care
- VAs would be provided with the discretion/choice to not provide HH care management for children in their Agency (in this case, it is anticipated the HH will contract with a downstream care manager to provide care management to children in Foster Care)
- In developing care plans, VAs providing HH care management will be required to comply with health care oversight mandates for children in foster care and meet the core care management requirements of the HH Program
- VAs providing care management may contract with HH to provide care management for children who are not placed in foster care or who were formerly in Foster Care
- HH and VAs will be required to establish agreements to ensure transitional arrangements are in place for children that transition in and out of Foster Care
- DOH and OCFS have begun to develop webinars and in–person training sessions to provide Health Home care management training and define VA case worker and HH care management roles
Design Elements: Integrating Early Intervention and Health Home Program
- Stakeholders generally support the State´s approach to leveraging the expertise of EI service coordinators and HH care managers by having the EI initial service coordinator continue to facilitate initial enrollment and the Health Home care manager provide ongoing care management, including the integration of EI services in the child´s comprehensive care plan
- State has discussed approach with Early Intervention Council and the New York State Association of County Health Officials
- State is continuing to work with stakeholders to discuss how to "operationalize" approach, including:
- Establishing clear, documented guidance regarding the roles of the EI initial service coordinator and the Health Home care manager, including ensuring EI program requirements are met
- Training on the roles and responsibilities of EI service coordinator and HH Care Management, including procedures for transitioning from initial EI coordination to HH Care Management, EI program requirements, HH program requirements
- Will require separate State Plan Amendment and CMS approval
Status of CMS Discussions
- State Plan Amendment (SPA) required to reflect the design elements of the Health Home model for children including:
- Amending the Health Home eligibility criteria to:
- Include trauma and at risk for another condition
- Amend the BMI at or above 25 and to include comparable definition for children
- Use the CANS–NY to determine acuity
- Establish legacy rates for TCM and Waiver Programs
- Amending the Health Home eligibility criteria to:
- In September 2014, State had initial discussions with CMS and submitted informal, draft SPA
- In November 2014, the State discussed Health Home model for children with Substance Abuse and Mental Health Services Administration (SAMHSA)
- Discussions were positive and supportive
- Next Steps:
- Respond to CMS questions (mostly technical)
- Submit formal HH SPA for approval (per "sequencing" rules of CMS after the approval of the Health Home Resources ($190.6 million) Waiver SPA) – State is working to submit this week
- Submit EI SPA for approval
Operational Elements: Enrolling Children in Enrollment
- Stakeholders requested a phased–in approach to enrollment.
- The State is considering procedures for identifying children and making initial assignments to Health Homes. To facilitate referrals, the design of Medicaid Analytics Performance Portal (MAPP) will provide authorized users the ability to make referrals to a Health Home.
- System design, feedback loops, procedures for authorization are under development.
- Design must consider protecting PHI
- Considerations for developing a phase–in plan will include:
- The "readiness" of designated Health Homes to begin serving children,
- Identifying regions or populations of children under which to implement a phase–in approach
- Accommodating the costs in the global spending cap
- It is anticipated the phase–in plan would continue to reflect the conversion of:
- Children enrolled in OMH´s TCM Program to Health Home on October 1, 2015
- Children enrolled in the OCFS Bridges to Health Waivers, the OMH SED Children´s Waiver, and the DOH Care at Home I/II Waiver will receive their care coordination through Health Home care management beginning on January 1, 2016.
Operational Elements: Consent for Enrollment
- Children´s consent rules are complex and multi–faceted
- State Agency Partners, including representatives from their legal departments, have been working with Health Homes that requested to participate in the development of consent procedures and forms to develop an approach to obtaining consent for the enrollment of children in Health Homes and the appropriate sharing of protected health information of children enrolled in Health Homes with parents and network providers.
- The children´s consent will recognize both the rights of parents/guardians to consent to the treatment of their children (re: parental/guardian consent to provide care management services to their child) and the rights of minors to consent to certain services (e.g., family planning, HIV/AIDS, mental health services, substance abuse services), and in those circumstances, to withhold such treatment/services from their parents.
- The HIT technology requirements of the Health Home program (see Application) for Health Homes serving children also recognize the inability to segment electronic health care information and may require health information for minors be shared by non–electronic means.
- DRAFT consent forms are available on Department´s website
- More information will be provided on April 29, 2015 webinar
Operational Elements: Standards for Care Managers and Engagement
- Stakeholders generally supported establishing qualifications for care managers, while noting the need to preserve flexibility to make operational decisions that best reflect the mix of children served
- Given the desired approach to keep case load ratios as low as practicable, particularly for those children with more intensive needs (acuity level of high or that may be in HFW when implemented) and the level of experience required to meet the care management needs of this group, the State is requiring that care managers that serve children with acuity level of "high" as determined by the CANS–NY or in HFW when implemented have:
- A Bachelors of Arts or Science with two years of relevant experience, or
- A Licensed Registered Nurse with two years of relevant experience, or
- A Masters with one year of relevant experience.
- Health Home Care Managers providing services to:
- High acuity children (as determined by the CANS–NY as modified) would be required to keep their caseload mix predominantly to children of the High acuity level (and HFW when implemented)
- Medium and high acuity children (as determined by the CANS–NY tool as modified) will be required to provide two Health Home services per month, one of which must be a face–to–face encounter with the child.
- Standards for children enrolled in the Early Intervention Program (EIP) and receiving Health Home services through a provider approved under EIP, the following minimum qualifications for EIP service coordinators, as set forth in Section 69–4.4 of 10 NYCRR will apply
- A minimum of one of the following educational or service coordination experience credentials:
- two years of experience in service coordination activities as delineated in this Subpart (voluntary or part–time experience which can be verified will be accepted on a pro rata basis); or
- one year of service coordination experience and an additional year of experience in a service setting with infants and toddlers with developmental delays or disabilities; or
- one year of service coordination experience and an Associates degree in a health or human service field; or
- a Bachelors degree in a health or human service field.
- Demonstrated knowledge and understanding in the following areas:
- infants and toddlers who may be eligible for early intervention services;
- State and federal laws and regulations pertaining to the Early Intervention Program;
- principles of family centered services;
- the nature and scope of services available under the Early Intervention Program and the system of payments for services in the State; and
- other pertinent information.
- A minimum of one of the following educational or service coordination experience credentials:
Proposed 2016 Children´s Medicaid Managed Care Model
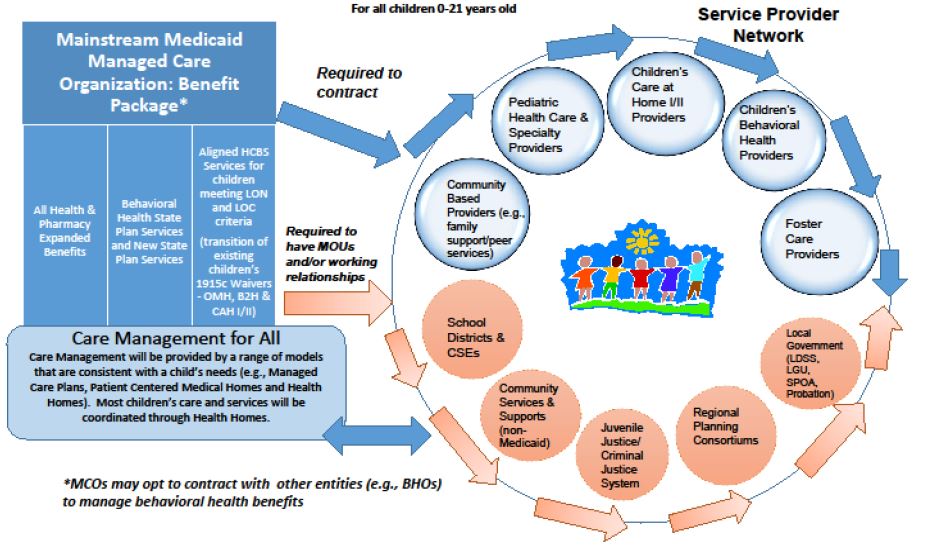
Design Elements
- Target Populations
- Children and youth younger than 21
- Children with Serious Emotional Disturbance (SED)
- Children in Foster Care who have SED, are Developmentally Disabled or Medically Fragile, or have experienced trauma
- Health Home important part of Children´s Managed Care Design
- Children who are physically disabled and require significant medical or technological health supports
- Youth with Substance Use Disorders
- Services
- Health Home for eligible children with chronic conditions, SED, Trauma (proposed) and Care management for LON children that don´t meet Health Home eligibility
- Expanded State Plan services
- HCBS services available to broader array of children
Proposed New State Plan Services
- Mobile Crisis Intervention
- Community Psychiatric Supports and Treatment (CPST)
- Other Licensed Practitioner
- Psychosocial Rehabilitation Services
- Family Peer Support Services
- Youth Peer Advocacy and Training
Proposed Menu of Home and Community Based Services
Children Eligible for Health Home will likely be eligible for HCBS (LON Criteria now under development)
- Care Coordination (only for those ineligible for, or opt out of, Health Home)
- Skill Building
- Family/Caregiver Support Services
- Crisis & Planned Respite
- Prevocational Services
- Supported Employment Services
- Community Advocacy and Support
- Non–Medical Transportation
- Day Habilitation
- Adaptive and Assistive Equipment
- Accessibility Modifications
- Palliative Care
Children´s Implementation Status
- Currently, work is focusing on:
- SPA review and SPA Provider Manual development
- SPA submission to CMS
- Developing HCBS Provider Manual, including evidence–based practices provider designation
- CANS–NY Revision, Testing and Implementation
- Health Home implementation for children
- Population and cost projections across service array
- 1115 development and submission to CMS
- Implementation scheduled for January 1, 2016
April 29, 2015
Webinar: Updates on Design Elements of Health Home Model for Children
- Update on SPA Submission Process
- HH eligible numbers
- MAPP Overview – Approach to Assignments/Referrals
- Rates
- Consent
- Background Checks
- Upcoming Trainings
- Updated Calendar with Key Dates
Resources, Questions and Answers
- State Partners are committed to working closely with Stakeholders to finalize the design of the Health Home model to serve children.
- Please send any questions, comments or feedback on Health Homes Serving Children to: hhsc@health.ny.gov
- Stay current by visiting our website: http://www.health.ny.gov/health_care/medicaid//program/medicaid_health_homes/health_homes_and_children.htm
- State Webinars, Training and Other Readiness Activities
