DSRIP Population Health Assessment:
Transforming the Health Care System
- Webinar is also available in Portable Document Format (PDF, 1MB)
PART 2
OFFICE OF HEALTH INSURANCE PROGRAMS
AUGUST 2014
We recommend reviewing Part I of this series:
DSRIP Population Health Projects:
Introduction to Population Health and Community Needs Assessment
June 2014
Office of Public Health
NYS Department of Health
Why is this community needs assessment different from all other community needs assessments?
- The goal of DSRIP is not to identify issues to be addressed within the context of the current health system.
- The goal of DSRIP is to transform the health care system by developing primary, preventive and other community–based care for Medicaid members to the level of efficiency that it results in a 25% reduction in avoidable hospital use (ED and hospital beds).
- This is not business as usual!
This Community Needs Assessment Is Different
- While the recently completed hospital community needs assessments, will likely have valuable information, they are not sufficient for this project.
- To achieve the goals of DSRIP, the solutions will be systems–based and not hospital–based.
- Health related resources, like community–based organization, will need to be assessed and included in planning to achieve goals.
- The findings of the DSRIP Community Needs Assessment (CNA) will drive the project selection process:
- The CNA should NOT be used to justify preselected projects the PPS wants to do or feels comfortable doing!
To transform a system, one needs to know the system …
STEP 1a: Understanding the Current System
The first step in the DSRIP Community Needs Assessment (CNA) is to identify the health and community resources that are available within the defined service area of the Performing Provider System (PPS).
- Health Care: This includes all of the medical and behavioral health providers within that system, even if not associated with the PPS at that time. Local Departments of Public Health, OASAS and OMH clinics should be included.
- Community Resources: This would include but not be limited to housing, food resources, advocates, peer organizations, etc. The CNA should consider unique resources such as community access computers in libraries.
For more information, please see the community needs assessment guide available on the DSRIP website.
STEP 1b: Understanding how the services come together
- How are these services currently connected and how could they be connected for ideal and efficient function? This includes an accounting of current services and actuarial analysis of specific future need. Actual realistic numbers will be expected in the CNA.
- What is the flow of services?
- Is there waste that could be removed without affecting quality?
- Would you want to receive services in the manner Medicaid members do?
- Where are services located in relation to critical populations?
- Are there transportation connectors?
- Are GeoAccess® like maps done?
- What important health sustaining services are missing in the area and how might available resources be reallocated or developed to address these missing resources?
- What are the identified redundancies including excess inpatient beds in the service area and how might these resources be reassigned/redesigned?
STEP 1c: Understanding the financial implications of change and how to rebalance
- How does the change in service structure impact financial stability of involved services? What are the plans for addressing these financial changes?
- How will PPS facilities address the expected reduction in hospital service use (emergency department and inpatient services, including reduction in excess bed capacity) and financially maintain appropriate tertiary care services?
- What is the potential for repurposing redundant facilities? What would be required to repurpose? Are there other community non–health needs that could be addressed such as housing?
- What are the financial implications of staffing changes to ensure appropriate redistribution, recruitment and retention? How will these be addressed?
Once the system is understood …
STEP 2: Understand the issues driving avoidable hospital use
- What health conditions in the Medicaid population are getting insufficient primary, preventive and community–based care?
- What chronic diseases are potentially preventable if these services were available?
- What social conditions are affecting the Medicaid population such that it affects compliance with medical and/or behavioral health treatment?
- Where are the disconnects in the health care system that affect continuity of care?
- Where are the resource gaps that are keep Medicaid members from achieving health?
- What are the language/cultural/ethnic considerations for the at–risk populations?
- What is the impact of literacy and health literacy?
- What are the strengths of the at–risk population that can be used to build a healthier community?
- Are these strengths (e.g., religious organization) included in community resources?
- Are there links that are or can be created to these resources?
Using data to understand the issues driving avoidable hospital use …
Decisions need to be driven by data …
The Department is making data available on the DSRIP website.
We strongly suggest that this be your initial primary source of data.
DSRIP Performance Chartbooks
Capital District
Adult Overall Composite
Prevention Quality Indicators (PQI90)
Medicaid Recipients, 2011–2012
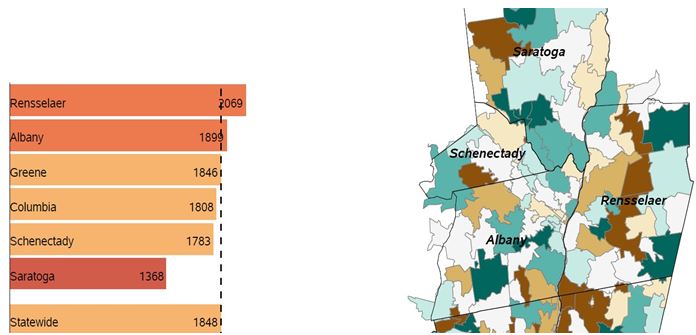
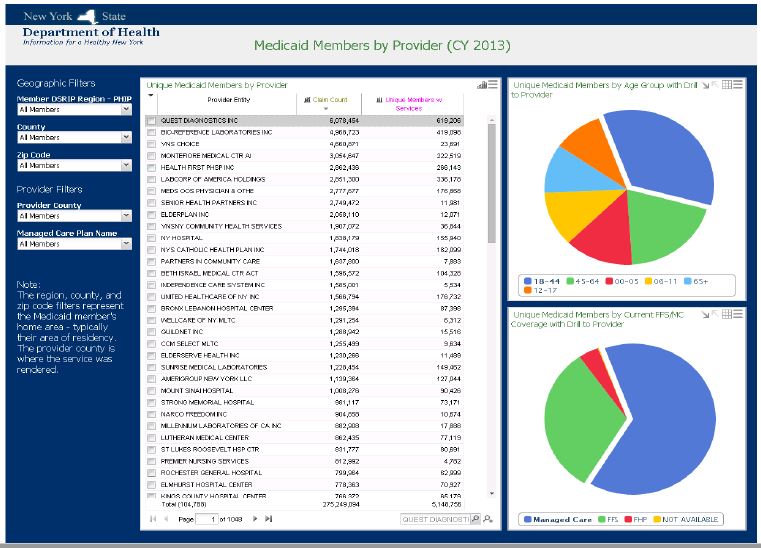
Salient Data Workbooks
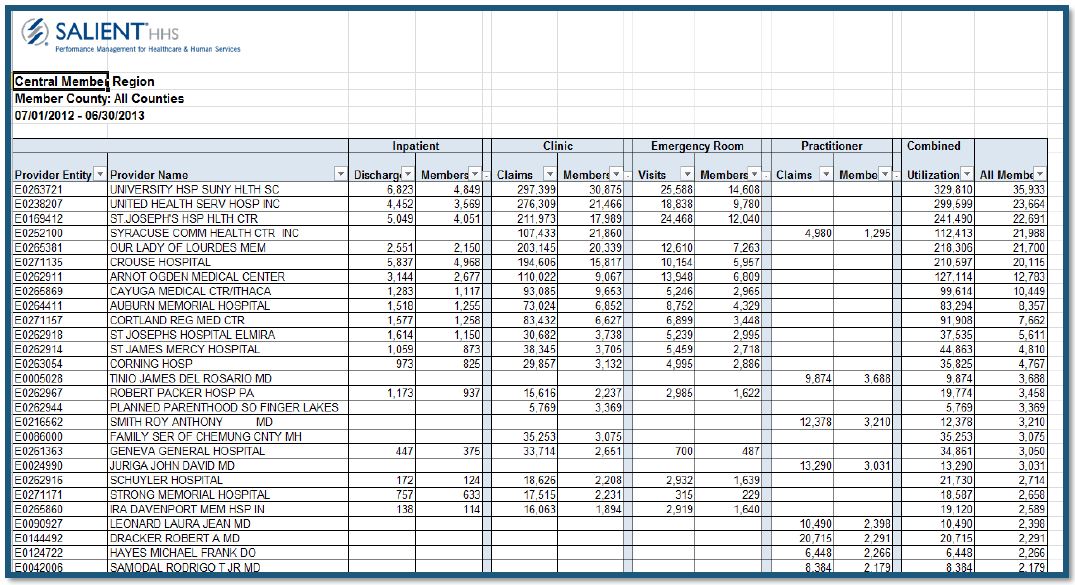
DSRIP Performance Dashboards
Web Based Performance Dashboards with drillable data on member counts by region and baseline performance data (PQIs, PPRs, etc.) are under development by Salient.
STEP 2: Understanding the issues driving avoidable hospital use…
- In addition to the data sources on the DSRIP website, there are numerous other sources of data including those collected by the PPS that can be used. Many of these are listed in the Part I of this webinar series.
- If using sources other than that provided by the Department, ensure the data is valid, reliable and reproducible.
The DSRIP Community Needs Assessment
STEP 3: Putting it all together
- The data collected during this comprehensive assessment should allow the PPS to define their community system and how it functions, the key populations affecting avoidable hospital use and the reasons why, and the appropriate data that will support its decision making.
- From the data, the PPS should be able to choose the appropriate projects to address the findings of the CNA.
- At the end of the CNA, the PPS will need to provide a completed spreadsheet in Excel that identifies the projects chosen for their DSRIP project, baseline data and justification for that selection.
DSRIP Project Plan Application
Tentative List of Community Needs Assessment Sub–Sections
- Summary of Health Care & Community Resources
- Current vs. Future State of Health Delivery System
- Methodology of Community Assessment Process
- Community Demographics
- Population Health Statistics
- Provider Demographics
- List of Community Needs
- Community Resources PPS Can Mobilize
- Stakeholder & Community Engagement
Questions?
We want to hear from you!
DSRIP website:
www.health.ny.gov/dsrip
DSRIP e–mail:
dsrip@health.state.ny.us
"Like" the MRT on Facebook:
http://www.facebook.com/NewYorkMRT
Follow the MRT on Twitter: @NewYorkMRT
Subscribe to our listserv:
http://www.health.ny.gov/health_care/medicaid/redesign/listserv.htm

Follow Us