Method
- Thoroughly document, using Worksheet B (PDF, 18KB, 2pg.), the characteristics of each disruptive behavior you are addressing, the circumstances surrounding its occurrence, its frequency and intensity to help reveal any patterns and/or environmental context for the behavior. Be sure to ask staff on all shifts to fill out Worksheet B to communicate their experience with the disruptive behavior in question to the past that worked to reduce or eliminate the behavior.
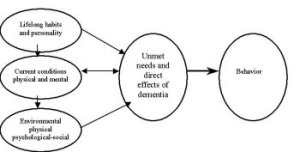
- Try to uncover any and all possible causes of the disruptive behavior) (PDF, 39KB, 2pg.). Each observed behavior should be systematically evaluated by: using MDS, resident or informant interview (family member, another or a previous caregiver in the nursing facility) to see whether the behavior represents a life-long habit or personality trait; appropriate medical, nursing, mental health or other professional(s) if there is a current physical or mental condition (chronic or acute illness, medication side-effect, dehydration, pain, sleep disturbance, etc.); or environmental factor (PDF, 400KB, 5pg.) that could be contributing to its occurrence.
The diagram below demonstrates how these factors contribute to produce disruptive behaviors:
- Look for clues in the results of step 2, above, that would indicate that the resident could be frustrated over limitations in sight, hearing or other sensory loses, reduced communication or cognitive skills (memory, behavior planning or problem solving), feel threatened by another resident or staff member, or is frightened by or responding to an overhead paging system or other stimulus in the environment that we take for granted.
- Identify activity (structured therapeutic recreation and normal daily activities of daily life) on all three shifts, seven days a week, during which the resident participates, seems to be content and focused, and where the disruptive behavior does not occur or is very infrequent. Identify particular caregivers and the care processes (e.g. bathing, dressing) that each provides when disruptive behavior doesn't occur or when it occurs to a lesser degree than usual. Document and share, using worksheet C (PDF, 21KB, 1pg.), with other team members how long the positive emotional state lasts and how long the disruptive behavior lasts when it occurs in these situations.
- If a consulting mental health specialist is used, prepare a summary of the information obtained in steps 1-4 above, to provide a comprehensive picture of the resident's problems and strengths that may provide clues about the nature of the resident's reactions in particular situations and the way the resident copes with anxiety, mood problems, etc.
- Develop and regularly conduct staff, family and resident education programs that explain disruptive behaviors as arising from unmet needs, confusion, emotional distress and other origins as you have identified them for particular residents in your setting. Inservice
- Evaluate the use of assigning compatible staff with whom the disruptive behavior tends not to occur so as to reduce disruptive behavior during specific care procedures.
- Follow the OBRA 87 mandate to use non-pharmacological intervention before using medication for disruptive behavior.
- Develop a Care Plan (PDF, 25KB, 1pg.) to address the disruptive behavior and evaluate the outcome (PDF, 33KB, 1pg.) of the approach (es) selected.
- Develop Facility Crisis Prevention Plan (PDF, 10KB, 1pg.) and Individual Crisis Prevention Plan (PDF, 126KB, 4pg.) so all staff are informed and trained about how to handle crisis before they occur. This is especially helpful for Aggressive Behaviors.
Approaches To Managing The Three Major Syndromes Of Disruptive Behavior (PDF, 14KB, 1pg.)
