Information Sheet: Health Consultation--Hudson River PCBs
Residential Proximity to the Hudson River and Hospitalization Rates for Ischemic Heart Disease and Stroke: 1990-2005
Westchester, Rockland, Putnam, Orange, Dutchess, Ulster, Columbia, Greene, Rensselaer, Albany, Washington and Saratoga Counties, New York
- The Information Sheet: Health Consultation--Hudson River PCBs is available in Portable Document Format (PDF, 387KB, 10pg.)
Background
The New York State Department of Health (NYS DOH) has a cooperative agreement with the federal Agency for Toxic Substances and Disease Registry (ATSDR) to conduct environmental exposure and health assessments and health studies for people in New York State who may have been exposed to environmental contaminants. This health consultation was conducted by NYS DOH in response to a request received by ATSDR in October of 2006. The request asked for follow-up on the findings of three research articles published in 2005-2006 that suggested residents living in ZIP codes along the Hudson River had higher rates of hospitalizations for cardiovascular disease (CVD) than other NYS residents. 1,2,3
A 200-mile segment of the Hudson River from Hudson Falls, New York, south to New York City is classified as a National Priority List (NPL) (Federal Superfund) site due to contamination of the river with polychlorinated biphenyls (PCBs) from General Electric sites in Hudson Falls and Ft. Edward (Washington County). The Superfund environmental investigations and remedial actions have focused on the areas of the river near Hudson Falls and Fort Edward where the highest levels of PCBs in sediments are located. The 2002 Record of Decision provides information about the human health risk assessment, conducted for the Upper and Mid-Hudson, and the ecological risk assessment, conducted for the Upper and Lower Hudson River.4 Fish contamination and fish consumption are the primary concerns at the site.
Some research has suggested that PCB exposures may cause biological effects that increase risks for heart disease, but there is very little research on human exposures to PCBs and potential cardiovascular effects. The widely known risk factors for cardiovascular disease (CVD) in addition to age, sex, race and family history, include tobacco use, high blood pressure, high serum cholesterol, alcohol use, obesity, low fruit and vegetable intake, physical inactivity, diabetes, low socio-economic status, mental ill-health, psychosocial stress and the use of certain medications. In the United States and in NYS, CVD rates are higher among people of lower socio-economic status. Because many risk factors for cardiovascular disease are associated with lower socio-economic status, it is especially important to adjust as much as possible for these differences when conducting comparative analyses of cardiovascular disease hospitalizations.
ATSDR and NYS DOH agreed to conduct a study using existing data from a statewide database on hospitalizations, following the same basic approach and statistical methods as the previous studies. The follow-up would attempt to improve on the prior studies by focusing on smaller geographic units than ZIP codes, census block groups. By using a level of geography that is generally smaller in area and population than a ZIP code, the follow-up study attempts to more thoroughly adjust for factors that affect cardiovascular hospitalizations and improve upon the assignment of relative distance to the Hudson River. Neither the prior studies nor this study conducted biological or environmental sampling as part of the study; distance to the river is the only information used to create the potential exposure categories.
Methods
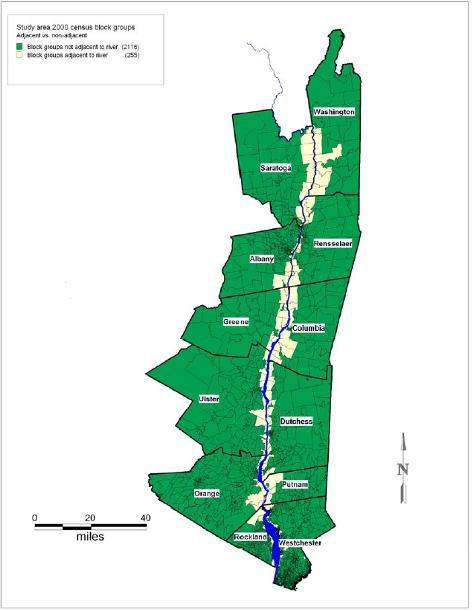
The follow-up includes the twelve counties along the Hudson River south of Hudson Falls (see map at right). Within these twelve counties, cardiovascular hospitalization rates in areas closest to the Hudson River are compared with rates in areas farther from the river while adjusting for factors such as sex, age and socio-economic status. This is a geographic approach that uses census block groups as the units of analysis, allowing rates per population to be calculated. To find out each hospitalized person's block group, each hospitalization address was first geocoded (placed on a computerized map).
The exposure assessment for this study is based on categories of distance to the river. Two types of distance categories were developed: adjacency and distance to the river shore. People in block groups directly along the Hudson River were assigned to the adjacent category, and people in all other block groups in the twelve counties were considered non-adjacent. For the distance categories, people were assigned to one of three categories based on the location of the block group: within ½ mile (closest), ½ to one mile (close), and farther than one mile (distant) from the shore of the river.
The follow-up evaluates the two main types of cardiovascular disease: ischemic heart disease, and two subsets, acute myocardial infarction (AMI - heart attack), and angina, pain in the chest; and cerebrovascular disease (stroke), and two subsets, ischemic stroke (blockage of blood flow to the brain) and hemorrhagic stroke (hemorrhage in an artery supplying blood to the brain). Hospitalization data from the Statewide Planning and Research Cooperative System contain information on each person's address, age, sex, race and diagnostic category. Population data from the United States Census (1990 and 2000) were used to estimate rates of cardiovascular hospitalizations per population by age, sex and race group for 1990 - 2005. Group-level census block estimates were used to assign additional information to each hospitalization. For example, each hospitalization was assigned the median income of the person's block group. Other information on education level, percent Hispanic, and population density was also assigned to each hospitalization using census block group estimates. Distance to the nearest hospital was also included in the models to try to account for mortality before reaching the hospital. These variables were used in multi-variable statistical models that compared hospitalization rates for populations in the various river distance categories while attempting to adjust for socio-economic and other differences among these populations.
Results
The use of block groups resulted in 2,371 block groups as the units of analysis for the study. In contrast, the study area contains 368 ZIP codes. The average population per block group in the study area is 1,200 compared to average population of 8,000 per ZIP code. The total study area population in 2000 was approximately three million. About eleven percent of the study area population is classified as living in block groups adjacent to the Hudson River and eighty-nine percent live in non-adjacent block groups. Eight percent of the study's population live in the closest block groups, ten percent in close block groups, and eighty-two percent live in distant block groups. The map shows the adjacent and non-adjacent block groups. The study includes over 150,000 hospitalizations, which represent a 50% random sample of the hospitalizations in the twelve counties over the study time frame of 16 years.
The bar chart below presents census data for 2000 and shows that populations in the different river distance categories also differ consistently in terms of race and ethnicity categories, education and poverty. The median income in 2000 for the closest block groups was $40,748, close block groups, $44,962 and most distant block groups, $64,847.
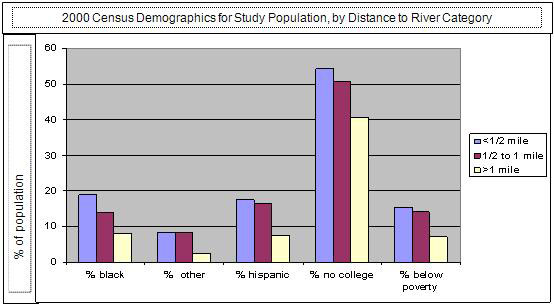
This association of lower income with living closer to the river creates a difficult challenge for this investigation because lower income is also associated with higher risk for cardiovascular disease. While the multi-variable analyses of hospitalization rates attempt to control for socio-economic differences, it will be difficult for any type of statistical modeling to disentangle the influences of socio-economic status and residential location on cardiovascular hospitalization rates.
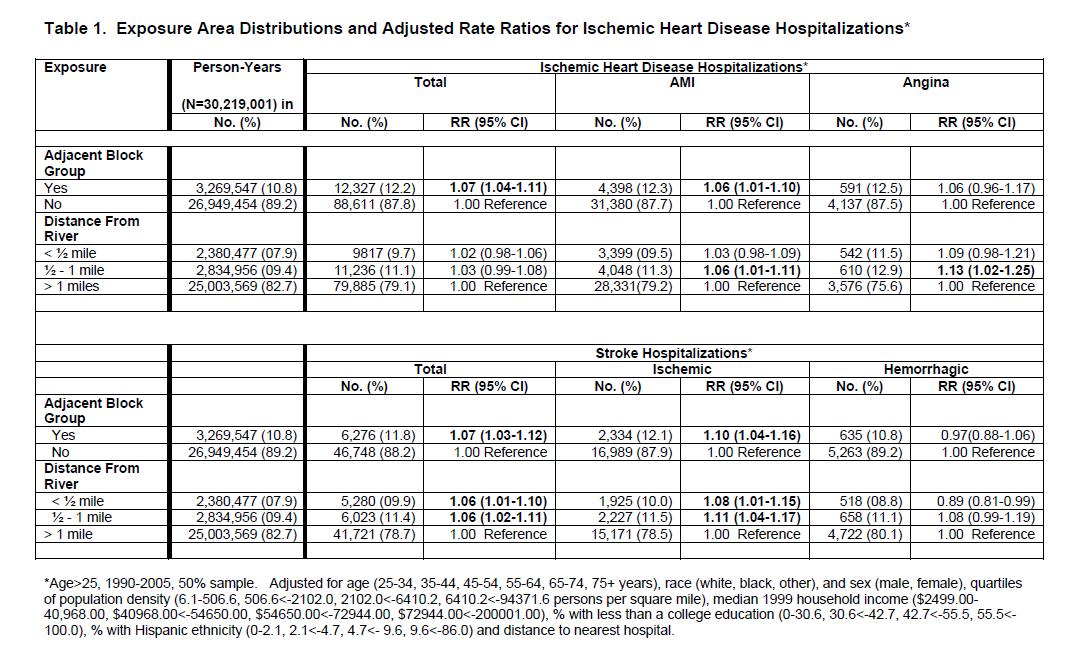
Table 1 shows the study's basic findings provided as rate ratios that compare hospitalization rates for populations living closer to the river to rates for populations farther away. A rate ratio of 1.00 indicates no difference and a rate ratio of 2.00 indicates a doubling of risk. The analyses show relatively small but statistically significant elevations of CVD hospitalization risk for residents of block groups categorized as adjacent, in close and closest proximity to the Hudson River. However, there is no evidence that residents of the closest block groups (within ½ mile) had higher hospitalization rates than residents of the close block groups (within one mile). If there were a strong association between exposures from living near the river and the risk of CVD hospitalization, such a "dose-response" might have been shown by the analyses.
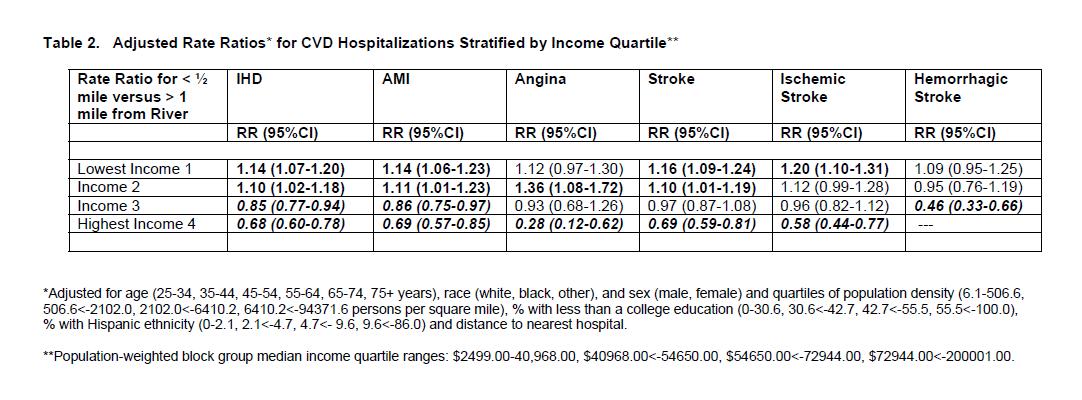
Because the analyses, consistent with other studies, show strong, statistically significant, associations between CVD risk and socio-economic status (results in full report), separate analyses for each of four income categories were conducted (Table 2). These analyses show that residence in block groups near the Hudson River is associated with increased risk for CVD hospitalizations among residents of lower income block groups but, conversely, residence in block groups near the Hudson River is associated with lowered risk for CVD hospitalizations among residents of higher income block groups. In other words, in analyses that held income constant by looking only within the lower or higher income populations, living near the river shows opposite effects depending upon which income group is considered.
This type of group-level statistical analysis is not able to precisely identify the reason for these differing results. However, the strength and direction of associations among variables in the statistical models can be evaluated in light of known risk factors to suggest likely explanations. In this case, socio-economic status appears to be the most likely explanation for the findings. The strong association between socio-economic status and residential location (the indicator of potential exposure) and between socio-economic status and CVD hospitalization risk makes it likely that the small but statistically significant elevations shown in Table 1 are the result of the inability to completely control for socioeconomic status' effects on CVD hospitalization risk.
Because of the similarities and differences in study design and analysis, the previously published studies' findings can be compared only to some degree with the findings of the current study. CVD hospitalization rate ratios estimated for living in block groups adjacent or near the river in the current study are substantially lower than the rate ratios for residence in ZIP codes adjacent to the Hudson River in the previously published studies. The rate ratios in the published studies ranged from 1.36 for ischemic heart disease, 1.39 for the subset, acute myocardial infarction (heart attack), a 1.20 for stroke, and 1.14 for hypertension. In most cases the current study's adjusted analyses show rate ratios lower than 1.10. The results of the current study are quite similar to the prior study results in terms of the associations reported for age, sex, race and income. These similarities and the general methodological similarities between the current and prior studies suggest that the prior studies' findings also were likely affected by uncontrolled socioeconomic status differences.
Discussion
Since 1976, fishing bans and advisories have been issued for the Hudson River because ingestion of fish is the major potential pathway for exposure to Hudson River PCBs for the general population. Previous studies have shown relationships between consumption of fish from contaminated waters and human PCB levels. Another potential pathway for exposure, less frequently studied to date, is inhalation of PCBs. NYS DOH and ATSDR launched "The Hudson River Communities Project" in 2000 to address this issue. This study gathered data on PCB levels in the environment and in people living in the Hudson River region with the highest potential exposures (Hudson Falls/ Fort Edward). The study detected a statistically significant reduction in the total PCB concentrations in outdoor air samples at a distance of 1200 meters (3/4 mile) from the River. However, the PCB levels in outdoor air in this area were lower than those in other communities with known PCB-contaminated sites, and similar to levels reported in other locations in the northeastern United States. The study found no detectable differences in study subjects' serum PCB levels associated with proximity to contaminated portions of the River or other PCB sources. 5,6
There are many other factors that affect CVD incidence, mortality and hospitalization risk that are not addressed in this short summary and which were not addressed in this study. One factor associated with potential PCB exposures that may play a role in the findings is the potentially higher consumption of fish contaminated with PCBs among lower income people living near the river than among higher income people living near the river. (This, however, would not help explain why higher income people near the River showed lowered CVD hospitalization risk than their counterparts living farther from the river.)
Group-level rather than individual-level analysis of CVD hospitalizations is a major study design limitation. This study used individual-level information on each hospitalized person's sex, race, age, and address, but information on other individual-level risk factors such as tobacco use was not available. River distance and other important characteristics such as education and income were assigned at the block group level, increasing difficulties of disentangling the effects of income versus residential location.
The study's other major limitation is the lack of group or individual-level PCB exposure assessment. Living near a body of water or hazardous waste site that contains PCBs or other contaminants does not necessarily mean that unusual human exposure has occurred. Neither the previously published studies nor this study included body burden or environmental sampling data in support of the categories used as indicators of potential exposure. This follow-up replicated the prior studies' geographic approach with some enhancements to attempt to better adjust for risk factors, particularly socio-economic status, which affect both residential location and hospitalization risk.
Conclusion and Recommendation
While this type of study can neither prove nor disprove causal links among risk factors and health effects, it is useful for examining evidence for unusual patterns that might warrant additional investigation. This evaluation revealed a closely coinciding pattern of lower socio-economic status and residential proximity to the Hudson River, and a strong association of lower socio-economic status and risk for CVD hospitalizations. These associations prevent us from drawing definitive conclusions from the multi-variable regression analyses.
In summary, the analyses showed relatively small but statistically significant elevations of CVD hospitalization risk for residents of block groups in close proximity to the Hudson River. Analyses conducted within each of the four income quartiles showed such elevations only among residents of lower income block groups. This study's data, methods and analyses can not provide a conclusive interpretation for this finding. However, the strong effect of socio-economic status on residential location (the indicator of potential exposure) and on CVD hospitalization risk makes it likely that the findings of elevations are the result of the inability to completely control for the effects of socio-economic status, a known risk factor for CVD.
To draw more definitive conclusions, particularly for outcomes such as CVD that are determined by multiple, known risk factors, studies seeking to investigate the role of PCB exposures will require resource-intensive methods that include gathering individual-level exposure or biomonitoring information as well as individual-level medical histories and information on other risk factors.
The results of the current investigation of CVD hospitalizations and residence near the Hudson River will be shared with NYS residents and other stakeholders with interest in this issue and will be submitted for publication in a peer-reviewed journal.
Additional Information
This fact sheet is a greatly abbreviated version of the full report. For copies of the full report, visit our website, call us at 518-402-7950 or 1-800-458-1158, or send an email to beoe@health.state.ny.us.
References
- 1Sergeev, AV and Carpenter DO. 2005. Hospitalization rates for coronary heart disease in relation to residence near areas contaminated with persistent organic pollutants and other pollutants. Environmental Health Perspectives, 113(6):756-761.
- 2Shcherbatykh I, Huang X, Lessner L, Carpenter DO. 2005. Hazardous waste sites and stroke in New York State. Environmental Health: A Global Access Science Source, 4(18).
- 3Huang X, Lessner L, Carpenter DO. 2006. "Exposure to persistent organic pollutants and hypertensive disease." Environmental Research, 102(2005): 101-106.
- 4United States Environmental Protection Agency (USEPA) 2002. EPA Superfund record of decision, Hudson River PCBs Site, Hudson Falls to New York City, New York. Washington DC
- 5Fitzgerald, EF, Belanger EE, Gomez MI, Hwang S, Jansing RL, Hicks HE 2007. "Environmental exposures to polychlorinated biphenyls (PCBS) among older residents of upper Hudson River communities." Environmental Research 104: 352-360.
- 6Palmer PM, Belanger EE, Wilson LR, Hwang SA, Narang RS, Gomez MI, Cayo MR, Durocher LA, Fitzgerald EF, 2008. "Outdoor air PCB concentrations in three communities along the Upper Hudson River, New York." Archives of Environmental Contamination and Toxicology, 54:363-371.
