DAL 16-05: Observation Services
DHDTC DAL 16-05: Observations Services
Dear Chief Executive Officer:
This letter is in follow-up to the New York State Department of Health's (Department) April 30, 2013 letter concerning statutory and regulatory changes to the governance of general hospital observation services (OS). This letter summarizes the provisions of a new section of Title 10 regulations, 405.32, which were promulgated to implement NYS Public Health Law 2805-v and 2805-w and became effective November 4, 2015.
Prior to November 4, 2015 OS were permitted via regulation, as outlined in the April 30, 2013 letter mentioned above. These amendments repeal those regulations, and create a new section 405.32, specifically for "observation services", which reflects the new state law and Center for Medicare and Medicaid Services (CMS) changes to oversight of OS, including allowing OS of up to 48 hours.
Any general hospital that is currently operating an OS program via a previously-approved Department waiver must be in compliance with the new regulations. If construction is required, the hospital has until November 3, 2016 -- within twelve (12) months of the effective date of the regulation-- to become fully compliant. The Department will be monitoring compliance.
The key provisions of the regulation include the following:
Organization/Policies and Procedures
- OS are defined as post-stabilization services appropriate for short-term treatments, assessments and reassessment of patients for whom diagnosis and a determination regarding inpatient admission, discharge or transfer can be reasonably expected within 48 hours.
- Direct referral to OS, bypassing the Emergency Department, is permitted, but is not required. The direct referral may come from a nursing home, hospital outpatient clinic, diagnostic or treatment center clinic, a physician or other appropriately licensed practitioner (nurse practitioner (NP) or physician assistant (PA). The referring practitioner should be a licensed physician, NP or PA who has conducted a physical assessment of the patient within the previous 8 hours from the referral.
- Policies & procedures must be developed and implemented whenever OS are established. These must cover organizational structure, location, clinical criteria, medical and administrative supervision, integration with related services, quality assurance and education/training of personnel. If direct referrals are utilized, detailed specific policies and procedures for this process must be established.
- The general hospital, in conjunction with its discharge planning program, must establish and implement written criteria and guidelines specifying the circumstances; the actions to be taken; and the appropriate contact agencies and individuals to accomplish adequate discharge planning for persons in need of post observation treatment or services, but not in need of inpatient hospital care.
- Each patient assigned to OS must be assigned a physician, NP or PA who will be responsible for the care of the patient and oversee timely discharge.
- Patients in OS shall be cared for by staff appropriately trained and in sufficient numbers to meet the needs of the patients.
Written and Oral Notice
- Written and oral notice must be provided to the patient or the patient representative within 24 hours of assignment to OS. The notice must include that the patient is not being admitted to the hospital and is being assigned to OS.
- The hospital must make a good faith effort to obtain written acknowledgment of the notice by the patient or the patient representative. If this is not obtained, the hospital must document its good faith efforts to obtain such acknowledgment, and the reason why the acknowledgement was not obtained.
- The notice must include a statement that OS status may affect the person's Medicare, Medicaid or private insurance coverage for the current hospital services, including medications and other pharmaceutical supplies, as well as coverage for any subsequent discharge to a skilled nursing facility or home and community based care.
- The notice must also indicate the person should contact their insurance plan to better understand the implications of being placed in OS.
Location
- OS may be provided in inpatient beds or in a distinct OS unit.
- There are no limits on the number of beds which can be contained in an OS unit or scattered throughout the hospital.
- Critical access hospitals authorized by Subpart F of Part 485 of Title 42 of the Code of Federal Regulations (CFR) or sole community hospitals, authorized pursuant to section 412.92 of Title 42 of the CFR, may also provide OS in an emergency department.
Distinct OS Units
- OS beds are not counted within the state certified beds of a hospital and are exempt from public need provisions of NYCRR Title 10 Part 709.
- The OS unit must be marked with a clear and conspicuous sign that states: "This is an observation unit for visits of up to 48 hours. Patients in this unit are not admitted for inpatient services."
Establishing a Distinct Observation Unit
Hospitals seeking to establish a distinct observation unit can accomplish this in two ways:
- When no construction is required, (as defined in subdivision 5 of section 2801 of the Public Health Law); no construction waivers are being requested; and no service is being eliminated, the hospital must notify the Department in writing, not less than 90 days prior to establishment. This notice must include the general location of the unit; the number of beds; and certification from a licensed architect or engineer that the space is compliant with applicable provisions of Part 711, 712-2 and 712-2.4 for construction projects approved or completed after January 1, 2011.
- When construction is required, (as defined in subdivision 5 of section 2801 of the Public Health Law); construction waivers are being requested; and/or a service will be eliminated, the hospital must submit a limited review certificate of need (CON) application, as per Part 710.1(c)(5).
- The observation unit must comply with the applicable provisions of 10 NYCRR Parts 711, Part 712-2 and 712-2.4 for construction projects approved or completed after January 1, 2011, except that the unit need not be adjacent to the emergency department.
The regulations can be accessed here:
Medicaid Payment Guidance
Medicaid covers OS. General billing guidelines for OS are articulated in prior publications:
- May 2011 Medicaid Update - Medicaid Begins Coverage for Hospital Emergency Room Observation Services:
http://www.health.ny.gov/health_care/medicaid/program/update/2011/2011-05.htm - February 2012 Medicaid Update - Health Department Regulations Adopted for Observation Unit Operating standards
http://www.health.ny.gov/health_care/medicaid/program/update/2012/2012-02.htm - May 2013 Medicaid Update - Observation Services Legislation and Medicaid Payment:
http://www.health.ny.gov/health_care/medicaid/program/update/2013/2013-05.htm
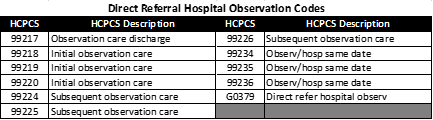
In order to bill under Ambulatory Patient Groups (APGs) for Direct Admit for Observation (DAO), the provider must be sure to include the following two procedure codes with the number of units and type of unit modifier indicated as follows:
- G0379 Direct Referral Hospital Observation (see full list of Direct Referral codes below); and
- G0378 Hospital Observation per hour, number of units (minimum of 8), and "UC" modifier if the service is provided in a designated Observation unit.
If both codes are present on the claim as well as an appropriate primary diagnosis, the Direct Referral Hospital Observation Code (which initially groups to APG 492) will automatically regroup to one of the following three medical APGs based on the primary diagnosis provided:
- APG 500- Direct Admission for Observation - Obstetrical
- APG 501- Direct Admission for Observation - Other Diagnoses
- APG 502- Direct Referral for Observation - Behavioral Health
Additional Billing Guidance
Facilities that do not have an emergency room rate code, can use their clinic rate code for billing. Facilities with both rate codes available for billing must use the emergency rate code.
The remittance will show the number of units and payment on the Direct Referral Hospital Observation (G0379) line and the Observation per hour (G0378) will package as follows:

If you have questions concerning Medicaid payment for OS, you should contact the Office of Health Insurance Programs (OHIP) at 518-473-2160. Inquiries concerning construction, or waivers from construction, should be directed to the Bureau of Architectural and Engineering Review at 518-402-0904. All other inquires may be directed to the Division of Hospitals and Diagnostic & Treatment Centers at 402-1004 or hospinfo@health.ny.gov.
Sincerely,
Ruth Leslie
Director
Division of Hospitals and Diagnostic & Treatment Centers
