Love Canal Follow-Up Health Study
"Love Canal Follow-Up Health Study, Spring 2006" is available in Portable Document Format (PDF, 1.48MB, 6pg.).
Love Canal Study Plan and Progress
Spring 2006
Serum Results Now Available
In 1999, the New York State Department of Health (DOH) began testing blood serum samples of nearly 400 individuals for levels of eight chemicals. The chemicals are known to be present at the Love Canal and were measured in soil and air from the surrounding community to make resettlement decisions. Measuring these chemicals in blood serum had not been done previously. Blood was drawn from Love Canal residents in 1978 and 1979 for routine medical blood tests. These blood chemistry tests were reported to the residents' doctors. The liquid part (called serum, or sera if more than one) of any leftover blood was saved for future use.
Beginning in 1999 we got residents' permission and began testing the stored sera to learn about chemical levels in residents who may have come into contact with chemicals at the Love Canal. The results provide a glimpse back in time about exposure by measuring levels of some Love Canal chemicals in blood for a cross-section of Canal residents. Unless people were further exposed to these chemicals after giving their blood sample, all but one of these chemicals would have been removed by their bodies years ago. The test results do not predict health effects from this exposure, tell us how the exposure happened or pinpoint the source of the exposure.
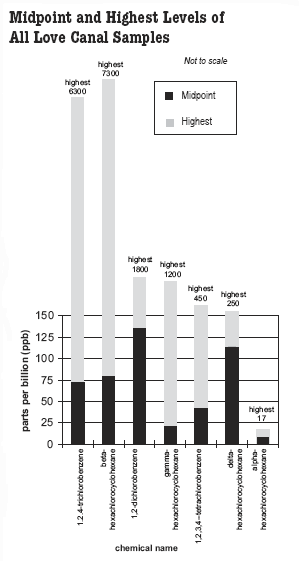
2-Chloronaphthalene was not detected The Love Canal Follow-up Health study has four parts: cancer, mortality, reproductive and serum studies. This article talks about the serum study which involves 373 residents. Each of them This table and the figure below show the range of serum levels found in the Love Canal group. The highest level of each chemical detected is shown as a gray bar on the figure. The midpoint values are shown as black bars. Serum normally contains some fats (also called lipids). A special process is used to extract (separate) the lipids from the serum and then the chemicals from the lipids. No extraction process works perfectly, and we accounted for that. This is what is meant by corrected for recovery. Therefore the results you see in this table and in the figure below are reported as the weight of the LCIC in nanograms per weight of lipid in grams, corrected for recovery, also sometimes called parts per billion (ppb). The Love Canal serum data are placed in the same format below. If the Love Canal group had no additional exposures to beta-HCH, and considering the years for the body to remove the chemical, we would expect the range of values from samples taken today to be about 1/12 of those in the table above, for a midpoint of about 6.4 ppb and a 95th percentile of about 26 ppb. We are in the final stages of completing the study. Most of the remaining work is reporting the results. Five reports are currently in process. The Agency for Toxic Substances and Disease Registry (ATSDR), who is funding the study, needed a report on our study efforts for the original grant. We discussed an outline for this report at a conference call in 2005 and included Committee and community representatives' suggestions in the first draft. The report consists of the preliminary mortality, cancer and reproductive findings that were already presented at Committee meetings and summarized in newsletters. It also contains something new - a discussion of those findings. ATSDR peer-reviewed the report and we are responding to the reviewers' comments. We expect this to be completed and approved by ATSDR sometime this summer. After peer review is finished, we will share the report with the Committee and release it for public comment. The next newsletter will summarize this report and invite your comments. We will also update you on further study funding, final reports and wrap-up plans (including a study wrap-up meeting) as these are developed with the Committee and ATSDR. You may recall that some of the preliminary study results indicated trends that merit closer evaluation. For example, in the years studied, more girl babies were born to Canal women than to mothers in the comparison population. This difference could be related to exposure or be due to chance alone. At the September, 2004 committee meeting and in a subsequent conference call, we discussed further exposure groupings that might be useful in clarifying the possible effects of chance or exposure in this observation. To capture as much statistical power from the data as possible, researchers are looking at the most common reproductive outcomes (birth weight and baby's sex) for possible associations with exposure groupings. This effort is leading to more analyses being incorporated into the cancer, mortality and reproductive evaluations. In addition to the ATSDR report, a report on each of the four studies will be submitted for publication in the science literature. Each report will be based on data presented to the Committee and discussed with community representatives. In addition, a summary of each report will be developed with the Committee and provided in future newsletters. The reports are in process: both mortality and cancer reports are nearly completed; reproductive analyses are nearly done, with report writing to follow; and statistical analysis of the serum results is underway. At our next conference call we will discuss how to structure the wrap-up meeting and final reports. Send any suggestions to Charlene Spampinato. As always, let us know if you want to be included in conference calls or receive meeting notices or minutes. Parts of the Love Canal Follow-up Health Study involve looking back to the time of exposure. Past exposure levels are being compared to current or past health effects to look for patterns. There is a possibility of error in assigning exposure levels to residents. We decided to measure actual chemical levels from as many stored samples as we could. These measurements will be compared to the exposure groupings already created and the health effects information already collected in the health study. The serum results do not tell participants how they were exposed or identify the source of exposure. They do not predict health effects and these levels are not expected to be present in the residents' blood today. The value of the serum study is to provide a marker for a person's exposure which can be compared to the assigned exposure grouping
for that individual and for the group they represent (Ring 1, residence near a hotspot, attendance at the 99th Street School, etc.). The results for the entire group of 373 residents might provide further insight into the relationship between health effects and exposure for the Love Canal community as a whole. Individuals who participated in the blood serum study are receiving their results with this newsletter. In 1978/79 the DOH Wadsworth Center Laboratory in Albany, New York received and stored any remaining blood serum left over from the blood collection at Love Canal in freezers. Over the past few years, as permission was obtained or we found out that a person had died, 391 serum samples from 373 people were tested for eight Love Canal Indicator Chemicals (LCICs). These same chemicals, chosen in 1985, were measured in soil to help decide whether or not to resettle the Canal neighborhoods. We know these chemicals are in the Love Canal and stay in the soil or air (not the human body) for a long time. We tested for the same chemicals in stored sera in this project. Serum normally contains some fats or lipids. The chemicals measured in this study are mostly found in the lipid part of blood serum. The amount of lipids in an individual's serum changes often and depends on many things, including his or her genetics, how recently the person ate or drank and what the person ate or drank. An individual with more lipids in his/her serum (for whatever reason) might be expected to have higher levels of LCICs in his/her serum than another individual even if they were both exposed to the same amount of LCICs. We know that no instructions were given about eating or not eating before bloods were drawn and we expect that some people ate and some did not eat. Differences in the amount of time between eating and the blood sample being taken may affect the LCIC levels since it affects lipid levels. We can help to account for this difference by adjusting the results for the amount of lipid present (expressed as percent lipid) in each sample. This is a usual procedure for blood analysis of chemicals. The actual process of testing for the chemicals in serum has many steps. One of the first steps in the measurement process is to separate the lipids and chemicals from the serum. We use a process called extraction to do this. A drip coffee maker uses an extraction in making coffee. When water is added to solid coffee grounds and the mixture is filtered, coffee is extracted out of the grounds. Laboratory extraction methods are much more exact, but the idea is still the same. After the extraction, the lipids are weighed. Another extraction is then used to separate the LCICs from the lipids. Then the weight of each LCIC in the sample is measured. The result is reported as the weight of LCIC (in nanograms) per weight of lipid (in grams). We tried different methods of extracting the serum and LCICs to choose the technique that best extracts the chemicals being measured in this study. No extraction process works perfectly. One way to account for this is to add a set amount of another chemical, called a surrogate, to each sample before extraction. We assume the LCIC is extracted as efficiently as the surrogate. We chose surrogates that are like the LCICs being measured and do not react with or change the levels of LCICs. (Two surrogates were used in the serum study - one that works well for chlorobenzenes and one that works well with hexachlorocyclohexanes.)
The amount of surrogate measured or recovered is compared to the amount originally added, and a percent is obtained. If 80% of the surrogate is measured after the extraction, we consider the extraction process to be 80% efficient. We then use the percent to adjust the LCIC measurements. The result is then reported as the weight of LCIC (in nanograms) per weight of lipid (in grams), corrected for recovery. These units can also be called parts per billion on a lipid weight basis, corrected for recovery, or parts per billion for short. If you have questions about any part of the Love Canal Follow-up Health Study, DOH researchers are available by phone, mail, fax or e-mail. Contact Charlene Spampinato:
in any of the serum samples. Almost all the sera had
some level of another chemical, 1,2,4-trichlorobenzene. The other
six chemicals were found in at least some of the samples. The results for
the group of Love Canal residents are summarized in the table
inside. Statistical analysis of the serum results will be
done as part of the Love Canal Follow-up Health
Study and reported in the future.
Serum Study: One Part of the Follow-up Health Study
Love Canal Indicator Chemical (LCIC)
Percent of samples with detectable levels
Levels for the Love Canal Group (ppb)
Lowest
Midpoint
Highest
1,2,4-trichlorobenzene
97%
3.3
73
6,300
beta-hexachlorocyclohexane
94%
8.6
77
7,300
1,2-dichlorobenzene
86%
6.4
130
1,800
gamma-hexachlorocyclohexane
49%
2.3
17
1,200
1,2,3,4-tetrachlorobenzene
28%
1.3
38
450
delta-hexachlorocyclohexane
5%
8.4
110
250
alpha-hexachlorocyclohexane
4%
2.5
6.7
17
2-chloronaphthalene was not detected in any samples
Survey Years
Midpoint
95th Percentile
1999-2000
Less than detection limit
69 ppb
2001-2002
Less than detection limit
43 ppb
Survey Year
Midpoint
95th Percentile
1978
77 ppb
309 ppb
Projected Value
Midpoint
95th Percentile
2006
6.4 ppb
26 ppb
Study Update
Serum Study Method and Purpose
For More Information
547 River Street, Room 316
Troy, NY 12180-2216
518-402-7530
Fax (518) 402-7539
E-mail: ceheduc@health.state.ny.us