NYS Heavy Metals Registry 2000 through 2005
- This report, New York State Heavy Metals Registry, 2000 through 2005, is available in Portable Document Format (PDF, 438KB).
Executive Summary
The New York State Department of Health (NYSDOH) Heavy Metals Registry was established in 1980 as a tool for the surveillance of adult exposures to arsenic, cadmium, lead, and mercury. Information is received from all clinical laboratories that test for any of these four metals in the blood or urine of adults who live or work in New York State. In 1992, legislation was enacted that required the reporting of all blood lead results, regardless of level. For mercury, arsenic and cadmium, only test results above specified limits are reportable to the NYSDOH.
This report presents statistics for the test results reported to the registry from 2000 through 2005. It is intended as a resource for programs providing preventive health care and for those concerned with reducing overall morbidity from heavy metals poisonings.
Only those adults (16 years of age and older) with reportable levels of arsenic, cadmium and mercury are added to the Heavy Metals Registry (See Appendix A for reportable levels). For this six year period, there were 899 adults with reportable levels of arsenic, 41 with reportable levels of cadmium and 7,952 with reportable levels of mercury. For lead, currently only blood lead levels of 10 micrograms per deciliter (µg/dL) or above are added to the Heavy Metals Registry. Overall, there were 12,522 adults with blood lead levels at or above 10 µg/dL.
NYSDOH staff routinely interview those adults with blood lead levels greater than or equal to 25 µg/dL (between 20 to 25 percent of all adults added to the Heavy Metals Registry for lead). Seventy-four percent of the people reported with blood lead levels greater than or equal to 25 µg/dL who were interviewed had an exposure that was occupational in origin. More than half of these occupational lead exposures were employed in the construction industry, and approximately 28 percent were employed in the manufacturing industry. Occupations reported in the Registry that had employees with higher blood lead levels included various construction trades, machine operators, laborers, precision production workers and assemblers. Due to high blood lead levels that have been reported to the Registry from employees in the scrap metal recycling industry, NYSDOH staff chose to examine this industry more closely. A study was conducted to identify and evaluate workers' exposures to lead and selected other hazardous metals in the scrap metal recycling industry. A summary of this study and recommendations to reduce workers' exposures are included in the Special Highlights section of this report.
Background
The New York State Department of Health (NYSDOH) Heavy Metals Registry (HMR) is a tool for the surveillance of adult exposures to arsenic, cadmium, lead and mercury. These metals are widely used in industry, and all have the potential to cause illness due to either acute or chronic exposure. Examination of the registry data can identify exposures in both communities and workplaces, thus allowing for early initiation of measures to help prevent exposures and potential illness.
The NYSDOH established the HMR in 1980 under Sections 22.6 and 22.7 of the State Sanitary Code (Appendix A), and reporting to the Registry began in 1982. All clinical laboratories, both in-state and out of NYS performing tests for arsenic, cadmium, lead and mercury on individuals residing or employed in NYS must report the results of the test to the NYSDOH. For mercury, cadmium and arsenic, only those tests above specified limits (shown in Appendix A) are required to be submitted to NYSDOH. From 1982 to 1986, blood lead levels of 40 micrograms per deciliter (µg/dL) or higher were reportable. In 1986, the reportable blood lead level was lowered to 25 µg/dL or higher. Then in 1992, as part of a major childhood lead poisoning prevention initiative, legislation was enacted to require the reporting of all blood lead results for all age groups, regardless of level. This legislative change has helped to identify elevated blood lead levels early and verify decreases in blood lead levels.
This report presents statistics for tests conducted from 2000 through 2005, and covers the four metals included in the HMR - arsenic, cadmium, lead and mercury. The number of adults reported since the inception of the Registry is presented for each metal. This report is intended as a resource for programs providing preventive health care and for public health officials concerned with reducing overall morbidity from heavy metals poisonings. Because of the change in the reporting requirement for lead in 1992 and because testing for lead exposure is much more common, lead tests account for approximately 78 percent of the tests added to the HMR each year. Therefore, the majority of this report focuses on the lead reports. The NYSDOH considers adult blood lead test results at or above 25 µg/dL to be indicative of an exposure to an identifiable source of lead, and conducts interviews on those adults.
This report also includes a Special Highlights section addressing lead exposure in the scrap metal recycling industry. This section discusses a study conducted by NYSDOH industrial hygiene staff that resulted in several recommendations for reducing lead and other heavy metal exposures for scrap metal recyclers.
Program Operation
Laboratories can report heavy metal test results electronically through the internet or manually on paper forms to the NYSDOH. All information reported to the registry is confidential, and records and computer files are maintained in accordance with NYSDOH regulations concerning medical data containing individual identifiers. Access to the data by anyone other than registry personnel is restricted and carefully monitored to ensure that confidentiality is maintained.
Registry staff contact all individuals reported to the registry with a reportable level of arsenic and cadmium. All individuals with reportable urine mercury levels are interviewed as well. Due to difficulty in identifying an exposure source for lower levels of blood mercury or lead and the absence of identifiable health effects at these levels, only those reports with blood mercury levels at or above 15 nanograms per milliliter (ng/mL) or with blood lead levels at or above 25 µg/dL are interviewed. Because of the large number of lead reports received each year, only those with blood lead levels greater than or equal to 10 µg/dL are added to the HMR. During an interview of a person reported to the HMR, the NYSDOH collects demographic information and information on the subject's work and home environments. This interview is used to determine the possible sources of exposure and to advise the person on appropriate control measures to limit future exposures. Subjects are provided with the local phone number of the NYS Occupational Health Clinic Network, for follow-up (Appendix B). When the exposure is work-related, information is gathered on the employer, work location, protective measures in place and whether coworkers are also potentially exposed.
Industrial hygiene staff provide consulting services to worksites with employees who have high or persistently elevated heavy metal levels. For situations where an employer has not previously had an employee who was reported to the HMR, an industrial hygienist contacts the company to determine the exposure circumstances, to learn whether coworkers are at risk, and to assess whether the company is taking appropriate measures to control exposures. With all contacts, the industrial hygienist protects the confidentiality of the individual reported. An important focus for these efforts is smaller businesses that do not have either full-time medical or industrial hygiene staff to evaluate their worksites. Between 2000 and 2005, there were 577 employers identified with at least one employee reported to the HMR with an occupational exposure to lead, 41 employers identified for occupational exposures to mercury, 11 for occupational exposures to arsenic and 2 for occupational exposures to cadmium.
NYSDOH staff make recommendations to employers on methods to reduce exposure to all heavy metals whenever feasible. The NYSDOH recommendations for exposures to heavy metals are guided by the federal Occupational Safety and Health Administration (OSHA) standards and the experience of the industrial hygienists in addressing similar exposures. The goal of the consultation is to identify site-specific exposure reduction techniques and to encourage monitoring to help assure that exposures have been reduced.
Arsenic
Figure 1. Number of Tested Adults Reported to the Heavy Metals Registry for Arsenic, by Year. The level of arsenic reportable to the Registry is 50 µg/L in urine. The number of reported adults tested for arsenic has remained relatively steady until 2000 when 109 adults were reported with urine levels of arsenic at or above 50 µg/L. This number increased to a high of 209 adults reported in 2002 and has declined to 149 adults reported in 2005. It is unknown why the number of reportable tests has increased so dramatically in the past few years.
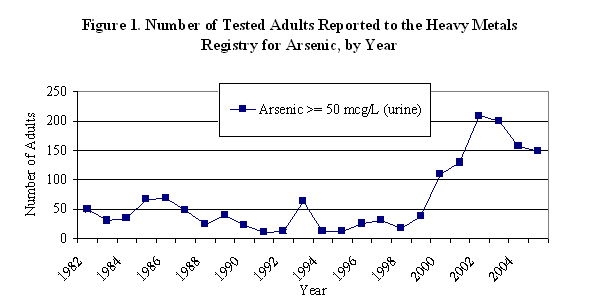
Table 1. Total Number of Tested Adults Reported to the Heavy Metals Registry by Sex, Age, Exposure Source, and Geographic Region for Arsenic, 2000 - 2005. Fifty-six percent of the adults reported each year were individuals over age 50, and almost 60 percent were male. For 80 percent of the adults reported with urine arsenic levels at or above 50 µg/L, the exposure source was non-occupational in origin. In general, non-occupational sources of arsenic exposure were attributed to seafood consumption. Organic arsenic, primarily from seafood is much less toxic to humans and not a health concern. Because most laboratories do not conduct speciation of a test (i.e., do not distinguish between organic and inorganic forms of arsenic), individuals are advised to avoid seafood consumption for two days prior to being retested. Very few individuals were reported with more than one arsenic result. It is unknown whether they are not being retested or if their levels upon retesting are no longer reportable (< 50 µg/L). The majority of the occupational exposures occurred among hazardous waste removal workers (data not shown).
Table 1. Total Number of Tested Adults Reported to the Heavy Metals Registry by Sex, Age, Exposure Source, and Geographic Region for Arsenic, 2000 -2005
| N | % | |
|---|---|---|
| Number of Adults | 899 | |
| Sex | ||
| Male | 535 | 59.5 |
| Female | 364 | 40.5 |
| Age | ||
| ≤29 years | 48 | 5.3 |
| 30-49 years | 342 | 38.0 |
| ≥50 years | 503 | 56.0 |
| Unknown | 6 | 0.7 |
| Exposure | ||
| Occupational | 10 | 1.1 |
| Non-Occupational | 719 | 80.0 |
| Both | 8 | 0.9 |
| Unknown | 162 | 18.0 |
| Geographic Area | ||
| NYS w/o NYC | 467 | 51.9 |
| NYC | 401 | 44.6 |
Cadmium
Figure 2. Number of Tested Adults Reported to the Heavy Metals Registry for Cadmium, by Year. The levels of cadmium reportable to the Registry are 10 ng/mL in blood and 5 µg/L in urine. The number of adults with reportable tests for cadmium has varied considerably since the registry began; however, there have always been less than 50 adults reported each year. Between 1995 and 2003, the number of adults with reportable cadmium levels has remained below five. The recent increase in adults with reportable levels appears to be principally due to occupational exposures, primarily among jewelers and casting machine operators (data not shown).
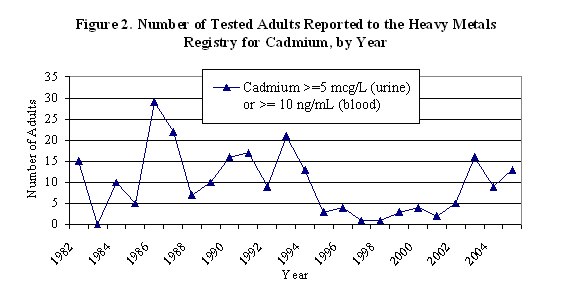
Table 2. Total Number of Tested Adults Reported to the Heavy Metals Registry by Sex, Age, Exposure Source, and Geographic Region for Cadmium, 2000 - 2005. Overall, between 2000 and 2005, there were 41 adults with cadmium levels reportable to the HMR. The majority of these were male (63%) and residents of upstate New York (all of NYS, excluding NYC). Despite being interviewed, the source of exposure was unknown for 44% of the reported adults.
Table 2. Total Number of Tested Adults Reported to the Heavy Metals Registry by Sex, Age, Exposure Source, and Geographic Region for Cadmium, 2000 - 2005
| N | % | |
|---|---|---|
| Number of Adults | 41 | |
| Sex | ||
| Male | 26 | 63.4 |
| Female | 15 | 36.6 |
| Age | ||
| ≤29 years | 5 | 12.2 |
| 30-49 years | 18 | 43.9 |
| ≥50 years | 18 | 43.9 |
| Exposure | ||
| Occupational | 12 | 29.3 |
| Non-Occupational | 11 | 26.8 |
| Unknown | 18 | 43.9 |
| Geographic Area | ||
| NYS w/o NYC | 27 | 65.9 |
| NYC | 11 | 26.8 |
Lead
Figure 3. Number of Tested Adults Reported to the NYS Department of Health for Lead, by Level, 2000 - 2005. Overall, there were 12,522 adults reported to the HMR between 2000 and 2005 with blood lead levels greater than or equal to 10 µg/dL. In 2000, 4,163 adults with blood lead levels of 10 µg/dL or above were included in the HMR; this decreased to 3,022 adults with blood lead levels of 10 µg/dL or greater in 2005. Also in 2000, 77,619 test results below 10 µg/dL were reported to NYS; this increased to 110,341 tests in 2005. Assuming one test per individual for those tests that are less than 10 µg/dL indicates that approximately 95 percent of all adults tested in 2000 had blood lead levels less than 10 µg/dL. In 2005, this increased to over 97 percent of all adults tested had blood lead levels less than 10 µg/dL. Females represented over 73 percent of those adults with blood lead levels less than 10 µg/dL (data not shown). Although New York State law does not require testing all pregnant women for blood lead, the state has established guidelines for health care practitioners to assist them in determining a woman's risk of lead poisoning on her initial prenatal visit. The high number of females with low blood lead levels could be a result of an increase in women getting pre-natal screening for lead exposure.
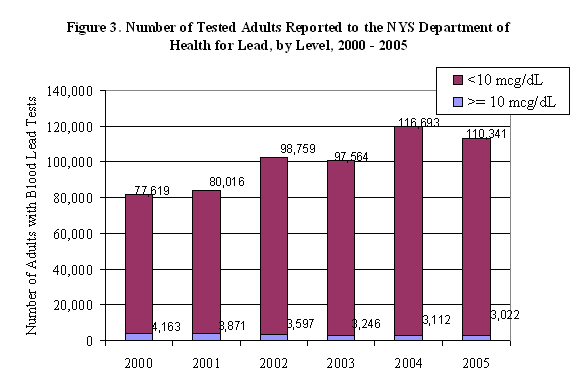
Table 3. Total Number of Tested Adults Reported to the Heavy Metals Registry With Blood Lead Levels ≥ 10 µg/dL, by Sex, Age, Exposure Source, and Geographic Region for Lead, 2000 - 2005. The results of all blood lead tests, regardless of level, performed on individuals residing or employed in New York State are reported to the HMR. Only those blood lead tests performed on adults (16 years and older) and with results at or above 10 µg/dL are added to the HMR. In 2000, 4,163 adults residing or working in New York State were tested for lead and had levels at or above 10 µg/dL. The number of adults tested with blood lead levels at or above 10 µg/dL has decreased annually to 3,022 adults in 2005 with levels at or above 10 µg/dL. The majority of the adults reported with blood lead levels greater than or equal to 10 µg/dL, for whom information is known, were middle-aged males.
Table 3. Total Number of Tested Adults Reported to the Heavy Metals Registry with Blood Lead Levels ≥ 10 µg/dL, by Sex, Age, Exposure Source, and Geographic Region for Lead, 2000 - 2005
| N | % | |
|---|---|---|
| Number of Adults | 12,522 | |
| Sex | ||
| Male | 10,021 | 80.0 |
| Female | 2,482 | 19.8 |
| Unknown | 19 | 0.2 |
| Age | ||
| <29 years | 3,425 | 27.3 |
| 30-49 years | 6,520 | 52.1 |
| >50 years | 2,537 | 20.3 |
| Unknown | 40 | 0.3 |
| Exposure | ||
| Occupational | 3,720 | 29.7 |
| Non-Occupational | 452 | 3.6 |
| Both | 74 | 0.6 |
| Unknown | 8,276 | 66.1 |
| Geographic Area | ||
| NYS w/o NYC | 6,771 | 54.1 |
| NYC | 4,447 | 35.5 |
Figure 4. Number of Tested Adults Incorporated into the Heavy Metals Registry for Lead, by Year. There were three distinct phases for the reporting of blood lead test results to the HMR attributed to changes in reporting requirements. From the start of the HMR in 1982 to 1986 (- -), only those tests greater than or equal to 40 µg/dL were required to be reported. From 1987 to 1993 (-
-), only those tests greater than or equal to 40 µg/dL were required to be reported. From 1987 to 1993 (- -), test results of 25 µg/dL and above were reportable. In 1992, a New York State regulation was enacted requiring the reporting of all blood lead results for all ages, regardless of level. This resulted in adding all reports with blood lead levels greater than or equal to 10 µg/dL to the HMR in 1994 (-
-), test results of 25 µg/dL and above were reportable. In 1992, a New York State regulation was enacted requiring the reporting of all blood lead results for all ages, regardless of level. This resulted in adding all reports with blood lead levels greater than or equal to 10 µg/dL to the HMR in 1994 (- -). Another contributing factor resulting in the increase in testing was the enactment of the OSHA Lead in Construction standard in 1993 requiring biomonitoring for construction workers with lead exposure. Each new reporting requirement resulted in an increase in the number of reports received. However, the number of adults added to the HMR with blood lead levels of 10 µg/dL or greater has steadily decreased since 1996, following the national trends of decreasing blood lead levels in adults and children.
-). Another contributing factor resulting in the increase in testing was the enactment of the OSHA Lead in Construction standard in 1993 requiring biomonitoring for construction workers with lead exposure. Each new reporting requirement resulted in an increase in the number of reports received. However, the number of adults added to the HMR with blood lead levels of 10 µg/dL or greater has steadily decreased since 1996, following the national trends of decreasing blood lead levels in adults and children.
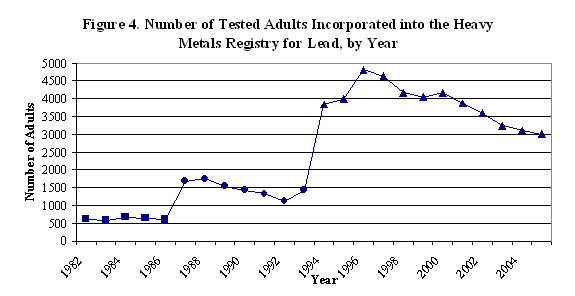
Figure 5. Percent of Tested Adults Reported to the Heavy Metals Registry with Blood Lead Levels ≥ 10 µg/dL, by Blood Lead Level, 2000 - 2005. Interviews are conducted on those adults with blood lead levels greater than or equal to 25 µg/dL. The NYSDOH considers adult blood lead test results at or above 25 µg/dL to be indicative of an exposure to a potentially identifiable source of lead. Therefore, interviews and interventions are conducted at this level and above. Consequently, the majority of lead reports in the HMR for those individuals with blood lead levels between 10 and 24 µg/dL have incomplete demographic information. Since 1996, slightly over 20 percent of all tests incorporated into the HMR (tests at or above 10 µg/dL) were greater than or equal to 25 µg/dL. Each year, the largest percent of blood lead reports added to the HMR are between 10 and 24 µg/dL. Of interest, is that even though the number of individuals with blood lead levels above 10 µg/dL has been steadily declining (Figure 6), the percent of those with levels above 25 µg/dL has been relatively steady. The remainder of this report will focus on those individuals with blood lead levels greater than or equal to 25 µg/dL.
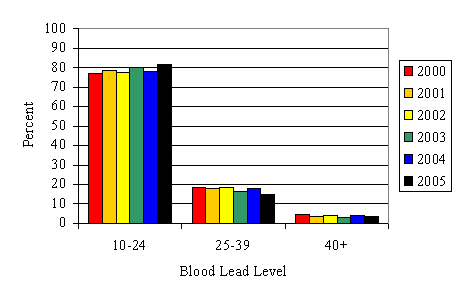
Table 4. Total Number of Tested Adults Reported with Peak Blood Lead Levels ≥ 25 µg/dL to the Heavy Metals Registry, by Sex, Age, Exposure Source, Geographic Region, and Blood Lead Level, 2000 - 2005. Over 90 percent of those adults reported to the HMR with blood lead levels at or above 25 µg/dL were men. Most of these men had blood lead levels between 25 and 39 µg/dL. The majority of all individuals reported with blood lead levels at or above 25 µg/dL were between the ages of 30 and 49.
Table 4. Total Number of Tested Adults Reported with Peak Blood Lead Levels ≥ 25 µg/dL to the Heavy Metals Registry, by Sex, Age, Exposure Source, Geographic Region and Blood Lead Level, 2000 - 2005
| Peak Blood Lead Levels (µg/dL) | ||||||||
|---|---|---|---|---|---|---|---|---|
| 25-39 | 40-59 | ≥ 60 | Total | |||||
| N | %* | N | %* | N | %* | N | %* | |
| Tested Adults | 2,161 | 564 | 76 | 2,801 | ||||
| Sex | ||||||||
| Male | 1,950 | 90.2 | 512 | 90.8 | 69 | 90.8 | 2,531 | 90.4 |
| Female | 211 | 9.7 | 51 | 9.0 | 7 | 9.2 | 269 | 9.6 |
| Unknown | 0 | 0 | 1 | 0.2 | 0 | 0 | 1 | 0.0 |
| Age | ||||||||
| <29 years | 493 | 22.8 | 116 | 20.6 | 15 | 19.7 | 624 | 22.3 |
| 30-49 years | 1,243 | 57.5 | 330 | 58.5 | 41 | 53.9 | 1,614 | 57.6 |
| >50 years | 421 | 19.5 | 118 | 20.9 | 20 | 26.3 | 559 | 20.0 |
| Unknown | 4 | 0.2 | 0 | 0 | 0 | 0 | 4 | 0.1 |
| Exposure | ||||||||
| Occupational | 1,590 | 73.6 | 436 | 77.3 | 47 | 61.8 | 2,073 | 74.0 |
| Non-Occupational | 270 | 12.5 | 78 | 13.8 | 20 | 26.3 | 368 | 13.1 |
| Both | 44 | 2.0 | 12 | 2.1 | 5 | 6.6 | 61 | 2.2 |
| Unknown | 257 | 11.9 | 38 | 6.7 | 4 | 5.3 | 299 | 10.7 |
| Geographic Area | ||||||||
| NYS w/o NYC | 1,201 | 55.6 | 288 | 51.1 | 35 | 46.0 | 1,524 | 54.4 |
| NYC | 703 | 32.5 | 224 | 39.7 | 35 | 46.0 | 962 | 34.3 |
| Out of NY | 231 | 10.7 | 44 | 7.8 | 5 | 6.6 | 280 | 10.0 |
| Unknown | 26 | 1.2 | 8 | 1.4 | 1 | 1.3 | 35 | 1.2 |
| *Note: Due to rounding, some percentage columns may not sum to 100. | ||||||||
Figure 6. Percent of Tested Adults Reported to the Heavy Metals Registry for Lead, by Occupational Status and Peak Blood Lead Level, 2000 - 2005. Seventy-four percent of reported lead exposures were occupational in origin with a high percent of those with blood lead levels below 25 µg/dL having an unknown source of exposure. Almost 13 percent of those with blood lead levels less than 60 µg/dL had a non-occupational source of exposure; while over 25 percent of those with blood lead levels greater than or equal to 60 µg/dL had non-occupational exposures.
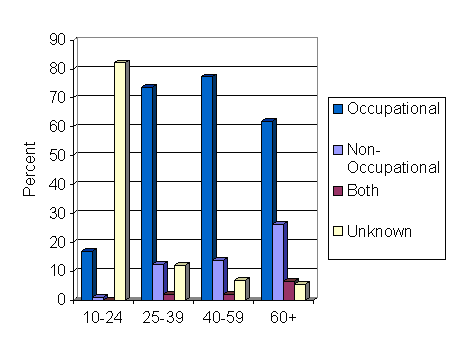
Figure 7. Number of Tested Adults Reported to the Heavy Metals Registry with Peak Blood Lead Levels ≥ 25 µg/dL, by Year and Geographic Area, 2000 - 2005. The number of individuals with blood lead levels greater than or equal to 25 µg/dL has been steadily declining in upstate New York. However, the number of individuals reported to the HMR with these blood lead levels from New York City has remained relatively steady for the past six years.
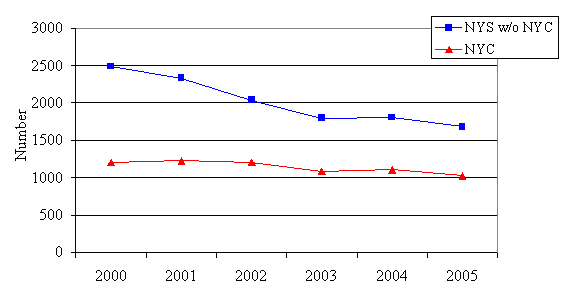
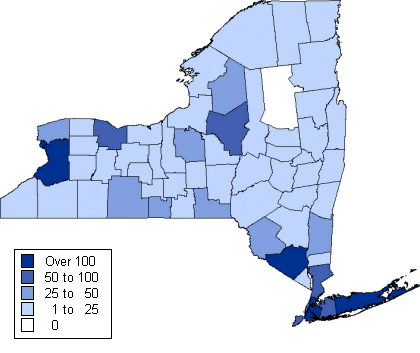
Figure 8. Distribution of Tested Adults Reported with Peak Blood Lead Levels ≥ 25 µg/dL, by County of Residence, 2000 - 2005. This figure displays the county of residence for individuals reported with blood lead levels greater than or equal to 25 µg/dL. In order to maintain confidentiality, the exact number of adults is not listed for those counties with three or fewer individuals reported with these blood lead levels. The data refl ect where individuals involved in lead-exposing industries or activities reside. (A large number of individuals are exposed to lead due to work in NYS, but reside elsewhere.)
Industry and Occupation
Table 5. Number of Tested Adults Reported with Occupational Exposures and Peak Blood Lead Levels ≥ 25 µg/dL, By Industry Type, 2000 - 2005. Occupational exposures includes exposures that are classified as occupational exposures only or both occupational and non-occupational. Only industries with more than three blood lead reports at or above 25 µg/ dL are included in this table. Over 58 percent of the occupational exposures occurred among individuals working in construction. Besides the construction industry, electronic and electrical equipment manufacturing and primary metal manufacturing industries have the highest number of individuals reported to the HMR with blood lead levels of 25 µg/dL or higher. These represent a few large employers in NYS who regularly conduct biomonitoring of their employees.
| SIC Code SIC Descriptor | Peak Blood Lead Level (µg/dL) | ||||
|---|---|---|---|---|---|
| 25-39 | 40-59 | ≥60 | Total | ||
| Construction | |||||
| 15 | General Contractors | 26 | 4 | 0 | 30 |
| 16 | Heavy Construction | 241 | 66 | 7 | 314 |
| 17 | Special Trade Contractors | 580 | 230 | 27 | 837 |
| Total | 847 | 300 | 34 | 1,181 | |
| Manufacturing | |||||
| 28 | Chemicals and Allied Products | 7 | 0 | 0 | 7 |
| 32 | Stone, Clay, Glass and Concrete Products | 79 | 9 | 0 | 88 |
| 33 | Primary Metal Industries | 160 | 15 | 1 | 176 |
| 34 | Fabricated Metal Products | 50 | 13 | 0 | 63 |
| 35 | Industrial Machinery and Equipment | 10 | 3 | 1 | 14 |
| 36 | Electronic and Other Electrical Equipment | 175 | 39 | 0 | 214 |
| 37 | Transportation Equipment | 3 | 1 | 0 | 4 |
| 38 | Measuring, Analyzing and Controlling Instruments | 3 | 0 | 1 | 4 |
| Total | 489* | 82* | 3* | 574* | |
| Non-manufacturing | |||||
| 48 | Communications | 9 | 2 | 0 | 11 |
| 49 | Electric, Gas and Sanitary Services | 40 | 4 | 2 | 46 |
| 50 | Wholesale Trade - Durable Goods | 21 | 4 | 0 | 25 |
| 55 | Automotive Dealers and Service Stations | 3 | 1 | 0 | 4 |
| 73 | Business Services | 8 | 0 | 1 | 9 |
| 75 | Automotive Repair, Services, and Parking | 10 | 0 | 0 | 10 |
| 76 | Miscellaneous Repair Services | 5 | 2 | 0 | 7 |
| 80 | Health Services | 4 | 0 | 0 | 4 |
| 87 | Engineering and Management Services | 7 | 2 | 0 | 9 |
| 92 | Justice, Public Order and Safety | 20 | 4 | 0 | 24 |
| 96 | Administration of Economic Programs | 22 | 1 | 0 | 23 |
| 99 | Nonclassifiable Establishment | 43 | 22 | 6 | 71 |
| Total | 205* | 46* | 10* | 261* | |
| *Totals do not add up correctly because only those industries with more than 3 cases are shown in table. Note: Table does not include 11 individuals with a known occupational exposure, but who did not have an assigned SIC code. |
|||||
Table 6. Number of Tested Adults Reported with Occupational Exposures and Peak Blood Lead Levels ≥ 25 µg/dL, by Selected Occupation, 2000 - 2005. Among individuals tested for occupational lead exposure, the occupations most frequently found in the Registry for reportable blood lead levels are the construction trades. In addition, machine operators, laborers, precision production workers and assemblers are found to be frequently reported occupations.
| Occupation | Blood Lead Levels (µg/dL) | |||
|---|---|---|---|---|
| 25-39 | 40-59 | ≥60 | Total | |
| Executive, Administrative and Managerial | 14 | 4 | 0 | 18 |
| Professional Specialty | 11 | 1 | 1 | 13 |
| Technicians and Related Support | 7 | 1 | 0 | 8 |
| Sales | 1 | 0 | 0 | 1 |
| Administrative Support, Including Clerical | 7 | 0 | 0 | 7 |
| Service | 40 | 8 | 1 | 49 |
| Farming | 2 | 0 | 0 | 2 |
| Mechanics and Repairers | 77 | 11 | 1 | 89 |
| Construction Trades | 688 | 244 | 31 | 963 |
| Precision Production | 58 | 13 | 1 | 72 |
| Machine Operators and Tenders | 158 | 39 | 1 | 198 |
| Fabricators, Assemblers and Inspectors | 62 | 13 | 1 | 76 |
| Transportation and Material Moving | 20 | 8 | 1 | 29 |
| Handlers, Equipment Cleaners, Helpers and Laborers | 136 | 35 | 7 | 178 |
| Total | 1281 | 377 | 45 | 1703 |
| Note: This table does not include 65 individuals with known occupational exposures, but who did not have an assigned occupation code | ||||
Table 7. Number of Tested Adults Reported with Non-Occupational Exposures and Peak Blood Lead Levels > 25 µg/dL, by Source of Exposure, 2000 - 2005. Many individuals with non-occupational exposures to lead never get tested for lead exposure. Individuals with these exposures often have the higher blood lead levels since they are presenting with symptoms resulting in them being tested. Blood lead levels above 40 µg/dL were identified in almost half of those reported with exposures to folk medicines, over a fourth of those with exposures from residential remodeling, and a fifth of those with exposures from target shooting.
| Blood Lead Levels (µg/dL) | ||||
|---|---|---|---|---|
| Exposure Source | 25-39 | 40-59 | ≥60 | Total |
| Accidental Ingestion, Pica | 31 | 9 | 3 | 43 |
| Cookware | 11 | 0 | 0 | 11 |
| Environmental* | 8 | 3 | 1 | 12 |
| Casting | 11 | 1 | 1 | 13 |
| Folk Medicine | 21 | 13 | 5 | 39 |
| Hobby, Jewelry, Crafts | 5 | 0 | 0 | 5 |
| Bullet Embedded in Body | 4 | 1 | 4 | 9 |
| Residential Remodeling | 68 | 22 | 3 | 93 |
| Target Shooting | 65 | 16 | 1 | 82 |
| Unknown | 46 | 13 | 2 | 61 |
| Total | 270 | 78 | 20 | 368 |
| *Environmental exposures are from lead in the environment around the household. These occurred outside of the United States. | ||||
Mercury
Mercury occurs naturally in the environment in several forms. A common form of mercury is called metallic or elemental. It is a silvery, odorless liquid that can evaporate at room temperature, becoming a vapor. Mercury can also combine with other chemicals to form inorganic or organic compounds. Urine and blood testing are the commonly accepted methods to assess mercury exposure for medical purposes. The type of test performed depends upon the nature of the suspected exposure. An elevated urine test for mercury indicates an elemental or inorganic source of mercury exposure. An elevated blood test for mercury indicates a recent exposure to a high concentration of mercury vapor or exposure to an organic mercury source (for example, methylmercury from a recent fish meal). Levels of mercury reportable to the Heavy Metals Registry are 5 ng/mL in blood and 20 ng/mL in urine.
Figure 9. Number of Tested Adults Reported to the Heavy Metals Registry for Mercury, by Year. In 2000, 482 adults were tested for mercury and reported to the HMR. The number of adults reported with these levels has increased dramatically to 2,810 adults reported in 2005. The number of reported adults tested for mercury previously peaked in 1986 with over 600 adults reported. The number then declined until 1994, remaining steady at less than 100 adults until 1998 when the number of adults with reportable mercury tests began to increase.
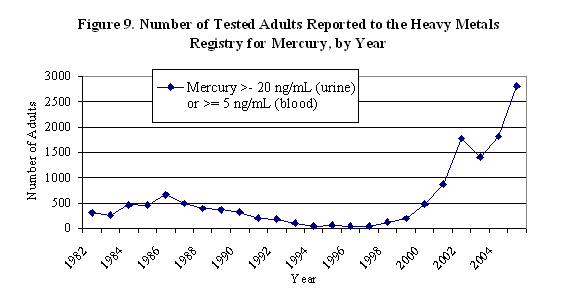
Figure 10. Number of Tested Adults Reported to the Heavy Metals Registry for Mercury, by Test Type and Year, 2000 - 2005. The increase in the number of adults with reportable mercury levels to the HMR is due to an increase in the number of reportable blood mercury levels received. In 2000, 97% of mercury tested adults were reported with blood tests. The percent of adults reported with blood tests has increased to over 99.5% of these reports. Based upon interviews conducted, this increase is attributed primarily to individuals whose exposure was through seafood consumption refl ecting an increase in testing of people who regularly consume seafood. Because of increased publicity regarding mercury in seafood, many individuals are now requesting these tests, and many doctors are now suggesting them.
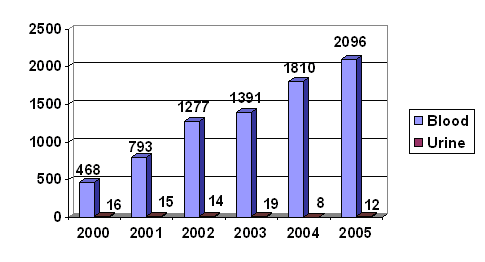
Table 8. Total Number of Tested Adults Reported to the Heavy Metals Registry by Sex, Age, Exposure Source, and Geographic Region for Mercury, 2000 - 2005. Overall, between 2000 and 2005, 7,952 adults were tested for mercury in 11,327 tests. These were almost equally divided between males (51.2%) and females (48.7%). Over half of those tested were residents of New York City.
Prior to 2000, all individuals reported to the HMR with blood mercury levels of 5 ng/mL or greater were interviewed. From those interviews, the NYSDOH determined that it is difficult to establish a source of exposure for blood mercury levels below 14 ng/mL and would find it difficult to provide advice and guidance on reducing or eliminating exposures. Also, in previous years, few adverse health effects were reported among those with blood mercury levels in this range. Therefore in 2000, the interview threshold was raised to those individuals with blood mercury levels of 15 ng/mL or higher. This level represents between 25 to 30 percent of all blood mercury test results received annually.
Interestingly, the number of reports attributed to known occupational exposures has been very low in recent years. In 2000, only 18 (3.7%) of the people tested for mercury had known occupational exposures, down from 11.3 percent in 1999 (data not shown). This number has decreased to only 2 individuals with occupational exposures (0.07%) in 2005. This reduction can primarily be attributed to fewer industries testing for mercury exposure rather than to a reduction in employee exposures. Since 2000, employees interviewed with occupational exposures to mercury worked in a variety of occupations, including dentists, laboratory workers/scientists, and public protection.
Table 8. Total Number of Tested Adults Reported to the Heavy Metals Registry by Sex, Age, Exposure Source, and Geographic Region for Mercury, 2000 - 2005
| N | % | |
|---|---|---|
| Number of Adults | 7,952 | |
| Sex | ||
| Male | 4,070 | 51.2 |
| Female | 3,872 | 48.7 |
| Unknown | 10 | 0.1 |
| Age | ||
| <29 years | 617 | 7.8 |
| 30-49 years | 3,664 | 46.1 |
| >50 years | 3,643 | 45.8 |
| Unknown | 28 | 0.3 |
| Exposure | ||
| Occupational | 63 | 0.8 |
| Non-Occupational | 1,889 | 23.8 |
| Both | 25 | 0.3 |
| Unknown | 5,975 | 75.1 |
| Geographic Area | ||
| NYS w/o NYC | 3,507 | 44.1 |
| NYC | 4,163 | 52.4 |
| Out of state | 0 | 0 |
| Unknown | 282 | 3.5 |
| Total Number of Tests | 11,327 | |
Special Highlights: Scrap Metal Recycling Industry Project
There were an estimated 5,785 metal recycling workers in New York State in 2000 (U.S. Census Bureau, County Business Patterns data http://censtats.census.gov/). Many of the materials or metals being recycled, such as ferrous and nonferrous scrap metals, vehicles and parts, communication cables, radiators, and batteries contain lead. From 1990 to 2000, the Heavy Metals Registry received reports of elevated blood lead levels (25 µg/dL or above) for 65 individuals working in metal recycling companies, one percent of the total estimated work force. Of those reported, 25 (38%) had blood lead levels above 40 µg/dL, and three (5%) had blood levels above 100 µg/dL. Based on these blood lead reports and the likelihood that the majority of the metal recycling workers may have not been tested, the true magnitude of the problem was unknown.
In order to learn more about the industry and the workers' lead exposures, the NYSDOH launched a Scrap Metal Recycling Industry project in 2000. The goals of the project were to collect information on metal recycling operations and processes from a representative survey population, to identify and evaluate workers' lead exposures in the scrap metal recycling industry, and to propose feasible and effective measures to reduce the exposures. NYSDOH worked with the Institute of Scrap Recycling Industries, Inc. (ISRI, a nationwide trade association for metal recycling companies) in developing the project. The project had two components - a mail survey and on-site industrial hygiene consultations; both were completed in 2001.
Mail Survey
A survey questionnaire was designed to gather information on company operations, potential employee lead exposures, and control measures being utilized, including personal protective equipment and biological monitoring programs. The survey population consisted of 224 establishments that were identified from statewide Yellow Pages' listings in the categories of "Scrap Metals", "Process & Recycle", "Scrap Metals & Iron (wholesale)", and "Steel-used". A total of 101 companies completed the survey, resulting in a response rate of 45 percent.
Industrial Hygiene (IH) On-site Consultations
On-site IH consultations were conducted by NYSDOH industrial hygienists at eight recycling operations that were representative of the entire sample based on the questionnaire findings. The industrial hygienists conducted a walk-through to observe recycling processes and employees' work activities and reviewed company lead safety programs at each facility. Personal breathing zone (PBZ) air samples were collected to measure employees' exposure to lead dust and fumes. These samples were collected during the performance of the various job tasks, such as sorting metal, driving forklifts, operating shears and balers, torch-cutting metal, and crushing cars. Surface dust wipe samples were also collected for the purpose of assessing the extent to which surfaces throughout the facility (e.g., non-production areas) were contaminated by lead and other metal dust. Areas sampled included surfaces in lunchrooms, bathrooms and locker rooms. Wipe samples were also collected from workers' hands.
Significant Findings and Discussion
- Workers were exposed to lead when cutting not only painted scrap metal, but also unpainted and new steel.
The survey found that unpainted metal or even new steel can contain lead and workers may be exposed to airborne lead concentrations exceeding the Occupational Safety and Health (OSHA) PEL while torch cutting new steel. Lead can get into scrap metal in a number of ways: (1) as a contaminant in the base metal; (2) as an intended ingredient in some alloys; or (3) as a dust or chemical deposit on the surface rather than in the paint. A common misconception held by the metal recycling trade is that only painted or galvanized coatings contain lead. Unpainted metals are often mistakenly classified as "clean" or "lead free" by metal recyclers. Thus, many torch cutters working with unpainted or new steel do not use respiratory protection. Given the difficulty in predicting the specific and precise metal content of any piece of material, it is prudent to wear proper respiratory protection while torch cutting of any metal.
- Surface lead contamination was widespread at metal recycling facilities and lead dust was found in employee bathrooms, lunchrooms, and on workers' hands prior to eating.
During the metal recycling process, lead dust is generated and dispersed through the air, eventually settling on surfaces both inside and outside of the work area, and on workers' exposed hair, skin, clothes and shoes. Lead dust that is tracked into lunchrooms and other non-work areas can pose an ingestion hazard. Workers can also inadvertently bring lead dust home, potentially exposing family members. The site visits found that even if air lead levels are fairly low, workers may still be exposed to lead through ingestion if the facility is not kept clean of lead dust. It is critical that workers wash their hands thoroughly before eating, drinking or smoking in order to minimize their risk of ingesting lead. A shower facility with separate "clean" and "dirty" lockers can help prevent cross contamination between the work and nonwork areas and the workplace and workers' homes.
- Biological monitoring for lead was provided by only 15 percent of the companies surveyed.
According to the survey, 85% of the companies surveyed had not provided employees with biological monitoring (regular blood testing) for lead. Metal recycling workers are exposed to lead through both inhalation (i.e., airborne lead dust and fume generated by torch cutting) and ingestion. The site visits found that the surface lead dust contamination was wide spread in metal recycling facilities; it is prudent to assume that all the scrap metal handling areas and adjacent support areas, such as lunchrooms, bathrooms, and offices may have lead surface contamination. Personal air monitoring cannot assess the extent of the workers lead exposure through ingestion and the only method to assess exposure from both inhalation and ingestion is biological monitoring.
- Companies tended to underestimate the degree and sources of lead exposure resulting in inadequate lead protection programs.
Our survey found that the greater the employer's awareness of workplace lead exposures, the greater the likelihood that the employer will conduct personal air monitoring and implement a biological monitoring program. However, at the time of the survey, 72% of the companies surveyed did not think that lead exposure was at least "possible" at their sites. This indicates that the owners of metal recycling companies may not realize the widespread nature of occupational lead exposures in their facilities. The information gathered through the survey indicates a need to educate employers within the metal recycling industry as to sources of lead exposure in scrap yard operations, risks of lead poisoning, and measures to prevent lead overexposure. Employers need to be aware of the requirements of the OSHA lead standard for general industry, and the importance of biological monitoring so they can take appropriate measures to protect their employees and to meet regulatory requirements.
Recommendations
The following recommendations were provided for scrap metal recyclers for their consideration:
- Implement engineering controls to reduce workers' lead exposures in scrap metal recycling operations;
- Provide employees with lead safety training;
- Institute a biological monitoring program to assess employee exposures to lead;
- Provide appropriate respiratory protection to workers who perform torch cutting, radiator disassembly, or any other tasks with the potential for significant airborne exposure;
- Provide hygiene facilities, such as a clean lunch room, and a locker room with separate "clean" and "dirty" lockers and a shower facility;
- Prohibit eating, drinking, and smoking in any area where lead contamination may occur, and require thorough hand washing before workers enter the lunch room, break area, or leave the facility; and
- Perform routine housekeeping to reduce surface lead dust accumulation throughout the facility.
Outreach and Ongoing Initiatives
Additional educational materials from this project are being developed to provide guidance to the metal recycling industry. These materials will be disseminated in collaboration with ISRI and the metal recycling companies that participated in the project. The NYSDOH will continue to monitor metal recycling workers through the Heavy Metals Registry and to conduct follow-up intervention activities. The goals of these intervention activities are to provide direct assistance to individual companies as needed as well as to monitor trends and changes in the industry. Updates to the guidance materials will be developed and disseminated as needed.
