Dental Care Survey, Medicaid Managed Care Members
- Document also available in Portable Document Format (PDF)
IPRO
Experts in Defining and Improving
The Quality of Health Care
New York State Department of Health
Office of Managed Care
February 2007
IPROCorporate Headquarters
Managed Care Department
1979 Marcus Avenue, First Floor
Lake Success, NY 11042-1002
516–326–7767 • 516–326–6177
TABLE OF CONTENTS
INTRODUCTION
Background
Objectives
METHODOLOGY
Population
Survey
Data Analysis
Methodological Considerations
- Response Rate Analyses
- Descriptive Results of Enrollee Survey
- Comparisons of Age Groups on All Enrollee Survey Items
- Predictors of Responses to Selected Survey Items
- MCO Variation
- Comparisons of Vendor Utilization on Enrollee Survey Items
- Comparisons of MMC and FFS Medicaid Groups
- Other Analyses
LIST OF TABLES
Table 1. Number of Adult Eligible Members and Surveys Mailed per Health Plan
Table 2. Number of Child Eligible Members and Surveys Mailed per Health Plan
Table 3a. Surveys Collected by Age Group
Table 3b. Response Rates for each Demographic Group by Payor
Table 4a. Number of Respondents and Response Rates for MMC Plans
Table 4b. Number of Respondents and Response Rates for FFS Medicaid Plans
Table 5a. Comparisons of Respondents and Non–respondents for MMC Members
Table 5b. Comparisons of Respondents and Non–respondents for FFS Medicaid Members
Table 6. Background Characteristics
Table 7. Oral Health Status
Table 8. Dental Care Information
Table 9. Barriers/Facilitators to Care
Table 10. Access and Availability of Dental Care
Table 11. Satisfaction with Dental Care and Health Plan
Table 12. Comparison of Children and Adults
Table 13. Significant Associations with Logistic Regression
Table 14. MCO Variability
Table 15. Comparison of MMC versus FFS Medicaid among Adults
Table 16. Comparison of Whites and Other Races
EXECUTIVE SUMMARY
Introduction
The purpose of this survey project is to assess the dental care that New York State Medicaid managed care organizations (MCOs) provide to their Medicaid enrollees, identify barriers to accessing care, and assess the satisfaction of recipients regarding dental care. This study was targeted to both members who receive dental benefits through their health plan and members whose dental care is paid via FFS Medicaid.
Poor oral health can impact children´s overall health, growth, school attendance, and can lead to medical complications. Dental caries comprises the single most common chronic childhood disease in the United States, and dental care remains the most prevalent unmet health care need for children. Several barriers to dental care have been identified, including lack of dental coverage, lack of adequate transportation, and a shortage of dentists willing to treat low–income, Medicaid, or disabled individuals. Significant disparities in the incidence and severity of oral diseases exist by race, income, education, disability status, homelessness, and migrant families.
Findings of the 2004 NYSDOH Medicaid Managed Care (MMC) Dental Provider Access and Availability Survey indicated that 53% to 89% of dentists/sites made appointments within the standard of 24 hours for urgent care and 28 days for routine care. These findings suggest that providers have open appointments, but they do not inform the extent to which members are actually visiting dentists, which is better measured by QARR. QARR rates for the Annual Dental Visit measure in NYS are low, with rates of 38%, 44%, and 43% for measurement years 2003, 2004, and 2005, respectively.
Methodology
Three scannable mail surveys were constructed, one each for: adult members, parents/guardians of child members, and long–term care members (presented in a separate report). Key survey indicators included oral health status, dental care visit in the past 12 months, whether the member has a regular dentist, ability to make timely appointments, satisfaction with the dentist and the health plan, barriers and facilitators to receipt of care, and demographic characteristics.
The total number of surveys mailed was 9,600 surveys for the MMC group and 2,400 surveys for the FFS Medicaid group. The survey was distributed to members in March 2006 and re–sent to non–respondents in May 2006. Both English and Spanish versions were mailed to each member.
Results
Of the 12,000 surveys that were mailed, 1,553 (13%) were undeliverable, and 2,330 surveys were completed, yielding a response rate of 22.3%. The FFS response rate (26%) was higher than the MMC rate (22%). Response rates differed by health plan, ranging from 14% to 27% for the MMC cohort, and from 17% to 34% for the FFS cohort.
To determine the extent to which the survey findings are generalizable to the total population, members who completed the survey were compared with those who did not on demographic variables. Among both the MMC and FFS cohorts, members who completed the survey were older than members who did not. Among the MMC cohort, respondents were more likely to be female, white, SSI recipients, and NYC residents compared to non–respondents. Among the FFS cohort, respondents were more likely to be white and SSI recipients than were non–respondents.
Descriptive Results of Enrollee Survey
Age ranged from 18 to 65 among the 1,255 adult respondents, and from 4 to 17 among the 1,075 children. Among the combined age groups, 39% were male, 72% had at least a high school diploma, 33% were white, 33% black, 24% Hispanic, and 9% other. Oral health was reported to be excellent or very good by 32% of respondents, good by 34%, and fair or poor by 34%. One–third reported having tooth or gum pain in the past year.
The majority of members (64%) visited a dentist within the past year, while 47% reported going at least twice. Half said they went to the dentist as often as needed within the past year. The major reason they last visited the dentist was for a regular check–up or cleaning (58%), while 39% went for a tooth or gum problem. A total of 71% usually go to a private dental office for care, while 27% go to a health center, community clinic, or hospital outpatient department. Two–thirds reported that they have a dentist they see on a regular basis. Regarding dental care behaviors, 81% reported they brush their teeth at least twice a day, 55% visit a dentist at least twice a year, 61% have their teeth professionally cleaned at least once a year, and 40% floss regularly.
Overall, 62% reported at least one difficulty in seeing a dentist as often as needed. The most common barriers cited were afraid or nervous to go (15%), dentists called do not accept their insurance (14%), do not like dentists or their particular dentists (13%), it is difficult to schedule an appointment (12%), have to wait too long in the waiting room (11%), and have trouble getting transportation (9%). When asked what would help them see the dentist more often, 78% cited at least one facilitator. The most common were more dentists to choose from (32%), reminders to visit the dentist (31%), better communication about benefits from their health plan (24%), and more convenient office hours (18%).
Most members found their dentist based on their plan´s provider directory (45%) or a referral from a family member or friend (34%). When asked how long they usually have to wait for an appointment for a dental problem, 38% reported 3 days or longer. The usual wait for an appointment for a regular check–up was less than 1 month for 74% of the respondents, 1 to 3 months for 21%, and longer than 3 months for 5%.
Ratings of very or somewhat satisfied were 68% for wait to get an appointment, 74% for dental advice and for overall quality of care, 77% for office hours, 80% for convenience of location, 81% for friendliness/helpfulness of staff, and 82% for cleanliness of office. Satisfaction with health plans´ explanation of dental benefits was 56%, and satisfaction with the number of dentists to choose was 47%.
Comparisons of Age Groups on All Enrollee Survey Items
Children and adults were compared on each survey item. Children were more likely to be Hispanic, to have good oral health status, to receive appropriate dental care visits, and to be satisfied with dental advice and health plan´s explanation of benefits, and less likely to report barriers or facilitators to care than adults. No differences were found on the access and availability indicators.
Predictors of Responses to Selected Survey Items
Multivariate regressions were performed to identify predictors of dental visits in the past 12 months, problems with receipt of care, length of time to wait for a routine appointment, and satisfaction with care and with the number of dentists to choose from. Eight variables served as independent variables in each regression: age group, gender, race/ethnicity, education, NY region, whether have a regular dentist, usual place for dental care, and oral health status.
Members who have a regular dentist were more likely to report that they have visited a dentist in the past 12 months than were members who do not have a regular dentist.
Members who have a regular dentist and members who rated the health of their teeth/gums positively were more likely to say they have no difficulties than their counterparts. Members who were black, those who resided in NYC, and those whose usual place of care is at a private dental office were more likely to report that they receive a routine appointment within one month than their counterparts.
Members who rated their oral health positively were more likely to be satisfied with the overall quality of dental care received than those who rated their health negatively.
Members who were black, those with a regular dentist, and those who rated their oral health positively were more likely to be satisfied with the number of dentists to choose from than their counterparts.
MCO Variation
Variation among the 16 MMC plans was examined on each survey item. Items with the widest range in plan rates included race/ethnicity, whether usually receive dental care at a private office, and how members found their dentist. Moderate variation was found for how long members have to wait to get an appointment and for several satisfaction items, while oral health status and some dental care indicators varied less.
Comparisons of Vendor Utilization on Enrollee Survey Items
The 12 plans that used a dental vendor in 2005 were compared with the four plans that did not to assess differences on survey responses. Members from plans using a vendor were more likely to get care at a private dental office (75%) compared to members not using a vendor (64%). Those with a vendor were also more likely to have found a dentist via their provider directory and less likely to use a referral from a family or friend than those without a vendor.
Comparisons of MMC and FFS Medicaid Groups
The MMC cohort was more likely to be black and less likely to be white than the FFS cohort. Compared to the FFS cohort, the MMC cohort was more likely to report good oral health status, that they last visited a dentist less than a year ago, that they visited a dentist at least once in the past year, that they usually go to a private dentist office, and that they usually wait less than one month for a routine appointment. The FFS Medicaid cohort was more likely to report that they choose their dentist based on referrals from family or friends. No differences appeared on barriers/facilitators to dental care or satisfaction with care.
Racial Disparities in Barriers and Facilitators
Race was dichotomized as white or other, and the two groups were compared on each barrier to seeing a dentist and each facilitator. Compared to whites, other races were more likely to report that they forget to go and have trouble finding a dentist who speaks their language. Whites were more likely to report that the dentists they called do not accept their insurance. Similar results were revealed on facilitators to care. The other races were more likely to report that reminders to visit the dentist, dentists that speak their language, and education about good dental care would help them see the dentist, while whites were more likely to cite more dentists to choose from.
Differences between FFS Medicaid and MMC on Barriers and Facilitators
FFS Medicaid and MMC cohorts differed on only one barrier: FFS members were more likely to report transportation as a major difficulty in seeing the dentist. No differences appeared on facilitators.
Discussion
One in three respondents reported only fair or poor oral health and major problems in the past year. Oral health status was rated better for children than adults, but one in five children were reported to have had a major tooth or gum problem in the past year. Oral health status could potentially be improved with interventions that impact oral care behaviors and access to professional care. Self–care and regular professional visits and cleaning presents an opportunity for improvement. Education regarding the need for such preventive dental service can be helpful, but the barriers to accessing such care are likely multifactorial and require more than one intervention to achieve improvement.
The surveyed population reported higher annual visit rates than HEDIS rates; this could have been affected by response bias, since individuals who visited a dentist may have been more likely to complete the survey. Having a regular dentist was the single significant variable for increased likelihood of having visited a dentist in the past year and reporting no difficulties in seeing a dentist. Children had higher rates of dental visits than adults. Half of the respondents indicated that they did not see the dentist as often as needed, an unmet need more pronounced in adults. Attention to oral health by adult primary care providers, with education and referral, could potentially increase access to preventive dental services.
Reported barriers indicate the need for implementation of multiple strategies to affect improvement. A total of 62% of respondents reported difficulty in seeing a dentist as often as needed, including contacting non–participating dentists and fear of dentists. Individuals seeking care for urgent problems reported lower rates of timely access than those seeking routine care, which is consistent with more difficulty seeing a dentist reported by those with fair or poor oral health. Commonly cited facilitators to care included reminders, which could be generated by plans or primary care providers, and better communication about plan benefits; 16% were not aware that they had dental benefits. Educational interventions about plan benefits, how to access them, and locating participating providers could assist in decreasing barriers to care. Lack of coverage for needed services was cited often and may reflect a lack of education regarding benefits or unmet need.
A total of 74% of respondents reported receiving timely routine care appointments. Timely routine care was more likely among NYC respondents and those who obtain care in private offices, possibly related to numbers of participating providers or longer wait times in hospital or community clinics. More difficulty was reported for acute problems, with 38% waiting more than 2 days for acute care. Respondents´ perceptions of acute problems may not be comparable to the acute problems described in the Access and Availability survey, but there was considerable discrepancy between wait times for acute appointments in this study and the Access and Availability survey.
Waiting time for appointments, which could be even longer for those without a regular dentist who did not respond to this query, was the item with the highest rate of dissatisfaction. MMC members reported better rates of timely appointments for routine care than FFS members, but rates varied moderately among plans. Plans should evaluate their individual rates and assess possible plan specific barriers to timely care.
Low numbers and geographic maldistribution of participating providers treating Medicaid eligible individuals affect access to care. “More dentists to choose from” was the most commonly cited facilitator to care. Other barriers, such as difficulty scheduling and long wait times in waiting rooms, could be related to numbers of participating providers. Low reimbursement rates and administrative complexities have been cited as factors negatively impacting dental participation in Medicaid. Streamlining administrative processes could be beneficial in increasing provider participation.
Reported rates of satisfaction with overall care among respondents with a regular dentist were generally high. Satisfaction with health plans was lower, specifically for explanation of benefits and numbers of dentists to choose from. Educational initiatives about plan benefits offer opportunity for improvement; provider pool and availability should be further assessed.
MMC enrollees fared better for annual visits than FFS members, but variability among plans in several access and satisfaction areas presents opportunities for improvement. Plans should further assess specific rates for satisfaction, member access to provider information, and availability of participating providers. Efforts to encourage identification of a regular dentist, which is associated with increased annual dental visits and fewer difficulties seeing a dentist, could positively impact visit rates. Such efforts could include dissemination of plan provider and benefit information, and educational interventions regarding the need for regular dental visits.
The proportion of members by race/ethnicity varied widely by health plans. Black members were more likely to receive appointments within one month and to be satisfied with numbers of dentists. This could be related to particular plans´ characteristics.
Compared to whites, other races were more likely to report forgetting appointments and difficulty finding a dentist who speaks their language as barriers, and that reminders, education, and language appropriate dentists would facilitate care. Reaching culturally diverse populations can positively enhance utilization of dental services and should be part of improvement interventions. Whites were more likely to report that more dentists to choose from would facilitate care, which may be related to plan characteristics and/or geographic maldistribution.
The response rate of 22.3% was relatively low, particularly with the inclusion of English and Spanish surveys in each mail package. Although respondents differed from non– respondents on age, race/ethnicity, gender, NY region, and Medicaid aid type, the impact of the difference is most likely minimal, since there were large sample sizes, small demographic differences among the MMC cohort, and no differences noted in the comparison between the mail and telephone respondents. Furthermore, logistic regressions to determine the relationship of each demographic variable with each survey item yielded very few significant variables. Response bias is a potential limitation, in that members who responded were probably more likely to have visited a dentist than non–respondents, resulting in higher reported rates of care.
Recommendations
Educating Medicaid families on accessing the dental care system is necessary, as a lack of knowledge about available resources has impeded access to care. Plans could develop interventions to ensure that members are aware of dental benefits, covered services, and how to access benefits and participating providers, and ensure that culturally diverse populations are reached. Education regarding routine care could be considered for inclusion in primary care visits. Increasing the number of members with regular dentists could improve access to ongoing guidance; this could be facilitated by member education regarding benefits and available providers and primary care provider referrals.
Analysis of plan specific participating provider pools, as well as geographic distribution of providers, could be an area for future study. Streamlining administrative procedures such as care approval processes has been cited as an intervention to enhance provider participation as well as care; plans should evaluate existing administrative procedures if believed to be a factor in accessing care.
Reminders to visit the dentist, generated by plans or primary care providers, could be implemented to facilitate care. Further analysis of lack of coverage for needed services should be conducted to determine if there is true unmet need or lack of knowledge about covered services.
|top of section| |top of page|INTRODUCTION
This study assesses the dental care of members participating in New York State Medicaid managed care organizations (MCOs). The primary purpose of this project is to provide the New York State Department of Health (NYSDOH) with information regarding the dental care that MCO enrollees receive, and to identify barriers to accessing care, and assess the satisfaction of Medicaid recipients regarding dental care. This study includes both members who receive dental benefits through their health plan and members whose dental care is directly paid via Medicaid, also referred to as FFS.
Background
Poor oral health can have a profound impact on children´s overall health, growth, school attendance, and social relationships, and can lead to medical complications. Dental caries comprise the single most common chronic childhood disease in the United States.1 Untreated tooth decay and the resulting pain and infection can cause eating, learning, and speech problems. Children with pain are more likely to be distracted at school and unable to concentrate on schoolwork. In adults, studies have found a correlation between severity of periodontal disease and risk of coronary heart disease, stroke, and a mother´s chance of delivering a pre–term, low–birth–weight baby. Poor oral health can have a long–term impact on a person´s appearance, self–esteem, and ability to find work.2
While tooth decay is one of the most preventable childhood diseases, dental care remains the most prevalent unmet health care need for children. Several barriers to dental care have been identified in the literature, including lack of dental coverage, lack of adequate transportation, and a shortage of dentists willing to treat low–income, Medicaid, or disabled individuals.
Significant disparities in the incidence and severity of oral diseases exist by race, income, education, disability status, homelessness, and migrant families. Children from families with low income, children in minority groups (e.g., black, Hispanic, and Native American), children of parents with low educational attainment, and children with special health care needs are more likely to have untreated dental caries, greater levels of dental disease, and are less likely to have regular dental care than their counterparts3, 12
In addition to a lack of dentists willing to serve Medicaid recipients, many Medicaid families may place limited priority on obtaining dental care, which also leads to low utilization of dental services. Low–income families have many competing needs, are sometimes unaware of the importance of oral health care and may be unwilling or unable to wait for appointments or arrange transportation to a dental appointment.
Other factors contributing to the disparity in care may be limited knowledge about oral hygiene and difficulty accessing preventive dental care.
The twin disparities of poor oral health status and lack of dental care are most evident among low–income children. These disparities continue into adolescence and young adulthood, but to a lesser degree. Other population groups served by Medicaid, including low–income adults, pregnant women, and disabled adults are also at risk.
In reviewing the 2004 NYSDOH Medicaid Managed Care (MMC) Dental Provider Access and Availability Survey findings, Medicaid members appeared to have some difficulty in making appointments within reasonable time frames. The findings indicate that 53% to 89% of dentists/sites made appointments within the standard of 24 hours for urgent care and 28 days for routine care. Note that these findings suggest that providers have open appointments, but they do not inform the extent to which members are actually visiting dentists, which is better measured by QARR/HEDIS.
HEDIS/QARR rates for the Annual Dental Visit measure tend to vary across the state and are uniformly low. The HEDIS Annual Dental Visit measure assesses the percentage of enrolled members who had at least one dental visit during the measurement year. In 2004, rates for 4 to 21–year olds in New York ranged from 10.5% to 53.0%, with a median of 41.5%, among the 20 Medicaid/Family Health Plus (FHP) MCOs that provided dental benefits. In 2003, the overall plan rate in NYC was 37%, and in the rest of the state, it was 43%. Overall, QARR rates were 38%, 44%, and 43% for measurement years 2003, 2004, and 2005, respectively.
In an attempt to assess this discrepancy between the high rates of availability and the varying Annual Dental Visit rates and to explore barriers and facilitators of dental care, this study surveyed Medicaid managed care members to identify any potential barriers in accessing care and assess the satisfaction and knowledge of Medicaid recipients regarding the dental care they receive.
Objectives
This study assesses the dental care of enrollees participating in New York State Medicaid MCOs. The major objective of this project is to serve as a quality improvement study providing the NYSDOH with information to identify barriers and facilitators of dental care. The study evaluated, from the patient perspective, the dental care that MCO enrollees receive, identifying barriers in accessing care, and assessing the satisfaction of Medicaid recipients regarding dental care.
The specific objectives of this project are to determine:
- Whether enrollees receive dental care in a timely manner
- Whether enrollees are satisfied with their dental care
- Barriers and facilitators to receipt of dental care
- Differences in the above indicators among demographic groups
- Differences in the above indicators between plan enrollees with dental care benefits and members enrolled in plans in which dental benefits are carved out to FFS Medicaid
To achieve these objectives, a survey instrument was created to address several components of dental care. Three scannable mail surveys were constructed: one for adult members, one for parents/guardians of child members, and one for long–term care members (presented in a separate report). Both an English and Spanish version were mailed to each member. Key survey indicators included dental care visit in the past 12 months, ability to make timely appointments, satisfaction with the dentist, and barriers to receipt of care.
A similar survey was also conducted of MLTC members, which is presented in a separate report and includes the same analyses, whenever applicable, that are included in this report for adults and children.
|top of section| |top of page|METHODOLOGY
Members from health plans serving Medicaid recipients in New York State were asked to participate in the survey. This study included both members who receive dental benefits through their health plan and members whose dental benefits are not covered through their plan but are directly paid via Medicaid. In the remainder of the report, the former group will be referred to as the MMC cohort, and the latter group as the FFS cohort. In order to maximize recall ability, the study included members who met the most recent eligibility criteria, allowing for membership lag.
Population
Inclusion criteria for the study population are as follows:
- Medicaid managed care enrollees and FHP enrollees
- Ages 4 to 65
- Continuously enrolled in the year 2005, with no more than one gap in enrollment up to 45 days
- Enrolled as of December 31, 2005
The NYSDOH identified all eligible members based on the selection criteria and provided IPRO with demographic (e.g., date of birth, gender, address) data for these members. Across the adult and child groups in the NYS Medicaid program, 1,149,021 members met these criteria. There were 517,968 eligible adult members and 631,053 eligible child members.
Sampling was performed differently for the MMC and FFS Medicaid populations. Among the MMC cohort, IPRO randomly sampled 300 adults and 300 children from each of the 16 Medicaid health plans with a dental care benefit. Among the FFS cohort, IPRO randomly sampled 100 adults and 100 children from each of the 12 corresponding health plans. Note that for this study, five health plans that offer a dental benefit in some counties were excluded from the FFS population (i.e., CarePlus, Community Choice, Fidelis, GHI HMO Select, and United HC–NY). These five were included in the MMC sample. GHI PPO was also excluded because it only had 7 eligible members across all ages. Fewer cases were sampled for the FFS cohort than from the MMC cohort, since no plan comparisons were performed for the FFS population.
Based on the sampling algorithm, the total number of surveys mailed was 9,600 surveys for the MMC group (i.e., 600 x 16 plans) and 2,400 surveys for the FFS Medicaid group (i.e., 200 x 12 plans). As seen in Tables 1 and 2, a total of 1,200 adults for the FFS cohort, 1,200 children for the FFS cohort, 4,800 adults for the MMC cohort, and 4,800 children for the MMC cohort were mailed surveys. It was expected that this number of cases would yield a sufficient sample to permit plan–specific analyses for the MMC cohort, as well as analyses for the overall FFS results and MMC/FFS comparisons.
Table 1. Number of Adult Eligible Members and Surveys Mailed per Health Plan
| Plan Name | Total* | FFS Medicaid | MMC | ||
|---|---|---|---|---|---|
| Total | Sample | Total | Sample | ||
| AFFINITY HEALTH PLAN | 37,337 | 37,337 | 300 | ||
| AMERICHOICE | 30,910 | 30,910 | 300 | ||
| CAREPLUS | 17,652 | 38 | N/A | 17,614 | 300 |
| CDPHP | 7,863 | 7,863 | 100 | ||
| CENTERCARE | 19,534 | 19,534 | 100 | ||
| COMMUNITY CHOICE | 2,479 | 930 | N/A | 1,549 | 300 |
| COMMUNITY PREMIER PLUS | 19,163 | 19,163 | 100 | ||
| EXCELLUS | 15,497 | 15,497 | 100 | ||
| FIDELIS | 43,020 | 12,495 | N/A | 30,525 | 300 |
| GHI HMO SELECT | 1,035 | 154 | N/A | 881 | 300 |
| GHI PPO | 7 | 7 | N/A | ||
| HEALTHFIRST | 59,616 | 59,616 | 300 | ||
| HEALTHNOW | 8,944 | 8,944 | 100 | ||
| HEALTH PLUS | 48,848 | 48,848 | 300 | ||
| HIP | 64,948 | 64,948 | 300 | ||
| HUDSON HEALTH PLAN | 5,500 | 5,500 | 300 | ||
| INDEPENDENT HEALTH | 6,992 | 6,992 | 100 | ||
| MANAGED CARE HEALTH | 445 | 445 | 300 | ||
| METROPLUS | 45,373 | 45,373 | 100 | ||
| MVP | 395 | 395 | 300 | ||
| NEIGHBORHOOD | 17,950 | 17,950 | 300 | ||
| NY HOSPITAL CHP | 13,495 | 13,495 | 300 | ||
| PREFERRED CARE | 3,646 | 3,646 | 100 | ||
| ST BARNABAS | 6,379 | 6,379 | 300 | ||
| SUFFOLK | 2,372 | 2,372 | 100 | ||
| TOTAL CARE | 3,928 | 3,928 | 100 | ||
| UNITED | 20,352 | 18,541 | N/A | 1,811 | 300 |
| UNIVERA COMMUNITY HEALTH | 2,665 | 2,665 | 100 | ||
| WELLCARE | 11,623 | 11,623 | 100 | ||
| TOTAL | 517,968 | 179,765 | 1,200 | 338,203 | 4,800 |
*Total = sum of FFS + MMC populations
Table 2. Number of Child Eligible Members and Surveys Mailed per Health Plan
| Plan Name | Total* | FFS Medicaid | MMC | ||
|---|---|---|---|---|---|
| Total | Sample | Total | Sample | ||
| AFFINITY HEALTH PLAN | 42,966 | 42,966 | 300 | ||
| AMERICHOICE | 34,600 | 34,600 | 300 | ||
| CAREPLUS | 25,200 | 28 | N/A | 25,172 | 300 |
| CDPHP | 12,357 | 12,357 | 100 | ||
| CENTERCARE | 25,233 | 25,233 | 100 | ||
| COMMUNITY CHOICE | 3,818 | 1,379 | N/A | 2,439 | 300 |
| COMMUNITY PREMIER PLUS | 20,075 | 20,075 | 100 | ||
| EXCELLUS | 23,007 | 23,007 | 100 | ||
| FIDELIS | 62,360 | 18,261 | N/A | 44,099 | 300 |
| GHI HMO SELECT | 594 | 157 | N/A | 437 | 300 |
| HEALTHFIRST | 67,709 | 67,709 | 300 | ||
| HEALTHNOW | 11,272 | 11,272 | 100 | ||
| HEALTH PLUS | 62,328 | 62,328 | 300 | ||
| HIP | 60,322 | 60,322 | 300 | ||
| HUDSON HEALTH PLAN | 10,682 | 10,682 | 300 | ||
| INDEPENDENT HEALTH | 9,303 | 9,303 | 100 | ||
| MANAGED CARE HEALTH | 322 | 322 | 300 | ||
| METROPLUS | 56,079 | 56,079 | 100 | ||
| MVP | 861 | 861 | 300 | ||
| NEIGHBORHOOD | 25,079 | 25,079 | 300 | ||
| NY HOSPITAL CHP | 12,293 | 12,293 | 300 | ||
| PREFERRED CARE | 6,212 | 6,212 | 100 | ||
| ST BARNABAS | 7,553 | 7,553 | 300 | ||
| SUFFOLK | 3,440 | 3,440 | 100 | ||
| TOTAL CARE | 6,245 | 6,245 | 100 | ||
| UNITED | 23,045 | 20,457 | N/A | 2,588 | 300 |
| UNIVERA COMMUNITY HEALTH | 3,521 | 3,521 | 100 | ||
| WELLCARE | 14,577 | 14,577 | 100 | ||
| TOTAL | 631,053 | 231,603 | 1,200 | 399,450 | 4,800 |
*Total = sum of FFS + MMC populations
Survey
A scannable survey was developed based on other existing surveys in the literature and previous NYSDOH surveys; additional questions were crafted as necessary. To obtain a comprehensive evaluation of dental care, several areas were identified for survey.
The questions were framed to explore oral health status, whether the member has a regular dentist, number of times visited dentist in the past 12 months, reasons for not going to dentist, accessibility of the dentist, satisfaction with dental care and the health plan, and demographic characteristics. All questions were written to a fifth–grade reading level. Because response rates for non–disease specific surveys tend to be low for this population, the survey was limited in length to maximize response rates.
Survey items included several formats, as follows:
- Dichotomous items such as yes/no.
- Multiple choice questions, consisting of three or more exhaustive, mutually exclusive categories.
- Likert–type questions to measure the direction and intensity of attitudes.
- Open–ended questions to explore the qualitative, in–depth aspects of a particular issue.
- Demographic questions to classify characteristics such as gender and race/ethnicity.
Two similar surveys were developed: one for adults and one tailored for parents/guardians of children. Questions in the two surveys were the same except that items in the children´s version referred to the child.
IPRO conducted two focus groups in January 2006 to ensure that members would understand the content and that the questions were relevant to the population and the survey was comprehensive. One focus group was for the long–term care members and the other for adult members. The surveys were altered slightly as a result of the comments from the attendees of the focus groups.
The survey was distributed to members in March 2006 and re–sent to non–respondents in May 2006 to maximize the response rate. Both English and Spanish versions were prepared and mailed in each package. Surveys were printed with randomly assigned identifiers used solely to track responses. Copies of the adult and child surveys are included in Attachments 1 and 2.
Participation in the survey was voluntary and confidential. Enrollees were told that it was optional to take part in the survey, that their answers would be kept strictly confidential, and that results would be reported in the aggregate. The survey included a sentence that directed them to call a toll–free number for assistance, if they needed it.
Data Analysis
Unless otherwise noted, all primary analyses were performed aggregating data for all enrollees, regardless of health plan. A focus of the analysis was to examine how enrollees receive dental care, and the perceived barriers to care. To explore whether care differs based on demographic characteristics, group comparisons were performed on selected key indicators for age group, gender, race/ethnicity, and other demographic characteristics. Analyses were also performed to explore plan rate variation. To test for any differences in proportions, chi–square analyses were employed for all comparative analyses.
The results section consists of 8 subsections. Specifically, the following areas of analyses were performed to address the objectives of this study:
- Response rate calculations of enrollee surveys, crosstabulations of response rates by age group; and response bias analyses (comparing respondents and non– respondents) on MCO, gender, age, race/ethnicity, and geographic region.
- Descriptive statistics on all survey items.
- Comparisons of age groups on all survey items.
- Predictors of responses to selected survey items.
- MCO variation on all survey items.
- Comparisons of vendor utilization on all survey items.
- Comparisons of MMC and FFS Medicaid on all survey items.
- Other analyses.
Sections A, B, and G included both the MMC and FFS Medicaid survey data. Sections C, D, E, F, and H only applied to the MMC respondents. MLTC survey data were reported in a separate document and will include the same analyses, whenever applicable, that are included in this report for adults and children.
Methodological Considerations
Because of the extensive number of indicators, many statistical tests were planned, thereby increasing the chance of a spurious statistically significant result. To limit the likelihood of reporting significance when it does not exist (type I error), the Bonferroni correction for multiple analyses was applied, resulting in an adjusted significance level of p<.001.
Due to the complexity of this survey, data manipulation was performed for analytical purposes. The following issues are discussed below:
- Items with multiple response options
- Skip patterns, with questionnaire items pertaining only to a subgroup of the sample
- Categorizing responses for crosstab analyses
Multiple Response Items
Three items on the survey asked the respondent to check all responses that apply, allowing the respondent to select multiple options. For such items, the total proportion of members selecting the corresponding options can sum to more than 100%. All proportions in this report are always based on the number of respondents, not the number of responses. For example, if 150 members answered a question with a total of 180 response options selected, the denominator was 150. These multiple response items are indicated in the tables with an "@" in the first column, and are listed below:
| Survey Item | |
|---|---|
| Q7 | Major difficulties had in seeing a dentist as often as needed |
| Q10 | How found dentist |
| Q15 | What would help see the dentist more often |
Items Pertaining Only to a Subgroup of the Sample
The survey contained one skip pattern, with some items based on a subset of the members who responded "Yes" to item 9. Items 10 through 13a were based on members who reported that they have a dentist to see on a regular basis. These items are denoted in the tables with a "◆".
Categorizing Responses for Crosstab Analyses
For statistical purposes, items that contained many response options were re–coded into fewer categories for all chi–square analyses. The descriptive results section (Section B), however, contains the raw frequencies of each item, and displays all options included in the survey. With the exception of questions 10 and 19, these items were dichotomized into two categories. The table below displays these items and the responses corresponding to each of the categories:
| Survey Item | Response Categories | ||
|---|---|---|---|
| Category 1 | Category 2 | ||
| 1 | Health of teeth/gums |
|
|
| 3 | Last time visited a dentist |
|
|
| 4 | Number of times visited a dentist in the past 12 months |
|
|
| 6 | Reason visited dentist last time |
|
|
| 7 | Major difficulties had in seeing a dentist as often as needed |
|
|
| 8 | Where usually go for dental care |
|
|
| 11 | How long usually have to wait for an appt. if have a dental problem |
|
|
| 12 | How long usually have to wait for an appt. if want a regular check–up |
|
|
| 13 | Satisfaction with dental care and health plan |
|
|
| 15 | What would help see the dentist more often |
|
|
| 18 | Education |
|
|
For item #19 (i.e., race/ethnicity), four categories were created (i.e., white, black, Hispanic, and other). The other race/ethnicity category included Asian, Native American, Arab, and Mixed Race. In the event that the respondent responded as Hispanic and any other race, the member was coded as Hispanic.
Note that, as is typical for survey research, whenever possible all "other" responses with open–ended text entered by the respondent, were re–coded to another existing response option that matched.
|top of section| |top of page|RESULTS
A. Response Rate Analyses
Table 3a displays the response rates, including the total number of surveys mailed and completed. Response rates were itemized by age group and by MMC/FFS sample.
Of the 12,000 surveys that were mailed, 1,553 (12.9%) were undeliverable, yielding an adjusted population of 10,447. The undeliverable rate is somewhat higher than other NYSDOH sponsored surveys of the Medicaid population, with undeliverable rates of 7.4%, 5.6%, and 7.6% in the Diabetes, Asthma, and ER Survey studies, respectively.
A total of 2,330 surveys were completed yielding an overall response rate of 22.3%. Among the completed surveys, 2,002 were in English and 328 were in Spanish. Across both age groups, the FFS response rate (25.7%) was higher than the MMC response rate (21.5%) at p<.001.
Table 3a. Surveys Collected by Age Group
| Children | Adults | |
|---|---|---|
| MMC | ||
| Surveys Mailed (Total Population) | 4,800 | 4,800 |
| Undeliverable | 529 | 627 |
| Adjusted Population | 4,271 | 4,173 |
| Completed Surveys | 864 | 952 |
| Response Rate | 20.20% | 22.80% |
| FFS Medicaid | ||
| Surveys Mailed (Total Population) | 1,200 | 1,200 |
| Undeliverable | 176 | 221 |
| Adjusted Population | 1,024 | 979 |
| Completed Surveys | 211 | 303 |
| Response Rate | 20.60% | 30.90% |
Response rates differed by health plan (see Tables 4a and 4b for MMC and FFS Medicaid, respectively), ranging from 13.9% to 26.8% for the MMC cohort, and from 17.1% to 34.3% for the FFS cohort.
Table 3b displays the response rates among the two payor groups (MMC and for FFS Medicaid) for each demographic group. Among the MMC cohort, females, SSI* recipients, and NYC residents were more likely to respond than their counterparts (i.e., males, SN or TANF recipients, and Rest of state residents, respectively). White and other race/ethnicities were more likely to respond than black members. Among the FFS Medicaid cohort, SSI recipients were more likely to respond than SN or TANF recipients. White members were more likely to respond than either black or other ethnicities.
Table 3b. Response Rates for each Demographic Group by Payor
| Field | MMC | FFS | |||
|---|---|---|---|---|---|
| Gender (among adults) | |||||
| Male | 20.0% | 28.1% | |||
| Female | 24.1% | 32.0% | |||
| Aid Type (among adults) | |||||
| SSI | 27.9% | 38.6% | |||
| SN or TANF | 22.1% | 27.9% | |||
| Race/Ethnicity | |||||
| White | 23.5% | 30.0% | |||
| Black | 18.9% | 19.7% | |||
| Hispanic | 20.9% | 21.3% | |||
| Other | 22.7% | 23.5% | |||
| Region | |||||
| NYC | 22.9% | 24.8% | |||
| Rest of state | 20.3% | 26.0% | |||
_________________________
* Note: SSI = Supplemental Security Income, SN = Safety Net, TANF = Temporary Aid to Needy Families.
Table 4a. Number of Respondents and Response Rates for MMC Plans
| Plan Name | Adults | Children | Total | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| AFFINITY | 43 | 17.5% | 26 | 10.4% | 69 | 13.9% |
| AMERICHOICE | 79 | 29.4% | 67 | 24.3% | 146 | 26.8% |
| CAREPLUS | 65 | 23.8% | 58 | 21.4% | 123 | 22.6% |
| COMMUNITY CHOICE | 69 | 27.1% | 46 | 17.5% | 115 | 22.2% |
| FIDELIS | 53 | 21.1% | 58 | 20.6% | 111 | 20.9% |
| GHI HMO | 62 | 23.3% | 35 | 13.8% | 97 | 18.7% |
| HEALTHFIRST | 43 | 17.5% | 53 | 19.6% | 96 | 18.6% |
| HEALTH PLUS | 61 | 22.2% | 57 | 20.7% | 118 | 21.4% |
| HIP | 61 | 23.7% | 58 | 21.6% | 119 | 22.6% |
| HUDSON HEALTH PLAN | 53 | 21.5% | 42 | 15.9% | 95 | 18.6% |
| MANAGED HEALTH | 52 | 19.5% | 49 | 18.5% | 101 | 19.0% |
| MVP | 53 | 22.4% | 52 | 21.5% | 105 | 21.9% |
| NEIGHBORHOOD | 71 | 24.9% | 56 | 20.1% | 127 | 22.6% |
| NY HOSPITAL | 76 | 27.8% | 51 | 19.2% | 127 | 23.6% |
| ST. BARNABAS | 58 | 21.4% | 77 | 28.2% | 135 | 24.8% |
| UNITED HC | 53 | 20.7% | 79 | 28.7% | 132 | 24.9% |
Table 4b. Number of Respondents and Response Rates for FFS Medicaid Plans
| Plan Name | Adults | Children | Total | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| CDPHP | 24 | 30.0% | 22 | 26.5% | 46 | 28.2% |
| CENTERCARE | 28 | 29.8% | 8 | 8.4% | 36 | 19.0% |
| COMMUNITY PREMIER PLUS | 29 | 32.2% | 26 | 29.2% | 55 | 30.7% |
| EXCELLUS | 25 | 32.1% | 16 | 20.0% | 41 | 25.9% |
| HEALTH NOW | 33 | 37.9% | 26 | 30.6% | 59 | 34.3% |
| INDEPENDENT HEALTH | 25 | 32.9% | 15 | 17.0% | 40 | 24.4% |
| METROPLUS | 22 | 25.0% | 23 | 24.7% | 45 | 24.9% |
| PREFERRED CARE | 30 | 37.0% | 12 | 16.2% | 42 | 27.1% |
| SUFFOLK | 18 | 25.0% | 9 | 10.5% | 27 | 17.1% |
| TOTAL CARE | 28 | 36.4% | 21 | 26.3% | 49 | 31.2% |
| UNIVERA COMMUNITY HEALTH | 18 | 24.0% | 15 | 18.8% | 33 | 21.3% |
| WELLCARE | 23 | 28.4% | 18 | 19.8% | 41 | 23.8% |
Response Bias
To determine the extent to which the survey findings are generalizable to the total population, a comparison was conducted between members who completed the survey with those who did not on age, gender, race/ethnicity, aid type, MCO, and NY region. Data for the members were obtained from NYSDOH databases. This analysis excluded the undeliverable surveys. Table 5a displays the results for MMC and Table 5b displays the results for FFS Medicaid, with column percentages for both respondents and non– respondents. The comparisons of respondents with non–respondents were tested with chi–squares and those which are statistically significant at p < .05 are identified, since the number of comparisons are few.
Because the demographic data apply to the actual member, and the child survey respondent was the parent, analyses for gender and age were restricted to the adult survey sample. Also, because virtually all children had an aid type of TANF, analyses for aid type were restricted to adults.
Among the MMC cohort, members who completed the survey were older than members who did not complete the survey, with mean ages of 39.7 and 36.6, respectively (via t– test; p < .05). This pattern is typical of survey studies and coincides with other survey response bias results. Respondents were more likely to be female, be SSI recipients, and NYC residents. Regarding race/ethnicity, respondents were more likely to be white and less likely to be black compared to non–respondents.
Among the FFS Medicaid cohort, members who completed the survey were older than members who did not complete the survey, with mean ages of 42.9 and 38.8, respectively (via t–test; p < .001). Respondents were more likely to be white and be SSI recipients and less likely to be black compared to non–respondents. The two groups did not differ significantly on gender or region (NYC versus Rest of state).
Table 5a. Comparisons of Respondents and Non–respondents for MMC Members
| Field | Groups | p value | |
|---|---|---|---|
| Responded (n = 1,816) |
Did not Respond (n = 6,628) |
||
| Gender (among adults) | 0.004 | ||
| Male | 258 (27.1%) | 1030 (32.0%) | |
| Female | 694 (72.9%) | 2191 (68.0%) | |
| Aid Type (among adults) | 0.004 | ||
| SSI | 142 (15.0%) | 367 (11.4%) | |
| SN or TANF | 807 (85.0%) | 2841 (88.6%) | |
| Race/Ethnicity | 0.0001 | ||
| White | 708 (39.0%) | 2303 (34.7%) | |
| Black | 572 (31.5%) | 2448 (36.9%) | |
| Hispanic | 144 (7.9%) | 544 (8.2%) | |
| Other | 392 (21.6%) | 1333 (20.1%) | |
| Region | 0.003 | ||
| NYC | 897 (49.4%) | 3016 (45.5%) | |
| Rest of state | 919 (50.6%) | 3612 (54.5%) | |
| Age (among adults) | |||
| Mean (standard deviation) | 39.7 (13.0) | 36.6 (12.5) | 0.0001 |
Table 5b. Comparisons of Respondents and Non–respondents for FFS Medicaid Members
| Field | Groups | p value | |
|---|---|---|---|
| Responded (n = 1,816) |
Did not Respond (n = 6,628) |
||
| Gender (among adults) | n.s. | ||
| Male | 74 (24.4%) | 189 (28.0%) | |
| Female | 229 (75.6%) | 487 (72.0%) | |
| Aid Type (among adults) | 0.001 | ||
| SSI | 108 (35.6%) | 172 (25.5%) | |
| SN or TANF | 195 (64.4%) | 503 (74.5%) | |
| Race/Ethnicity | 0.0001 | ||
| White | 306 (59.5%) | 715 (48.0%) | |
| Black | 110 (21.4%) | 447 (30.0%) | |
| Hispanic | 19 (3.7%) | 70 (4.7%) | |
| Other | 79 (15.4%) | 257 (17.3%) | |
| Region | n.s. | ||
| NYC | 136 (26.5%) | 413 (27.7%) | |
| Rest of state | 378 (73.5%) | 1076 (72.3%) | |
| Age (among adults) | |||
| Mean (standard deviation) | 42.9 (12.2) | 38.8 (12.1) | 0.0001 |
Telephone Follow–up of Non–Respondents
A telephone interview was conducted among mail non–respondents to assess the extent to which the survey findings are generalizable to the total population. Telephone interviews consisted of a shortened form of the mail survey containing four representative questions drawn from the survey and three additional questions to ascertain why they failed to respond. Since the intent was not to yield complete surveys, the number of questions was limited to help increase the likelihood that phone respondents would participate. Interviewers telephoned a random sample of non– respondents shortly after the mail phase was concluded. The random sample of 1000 adult members was selected from the pool of non–respondents, after removing FFS Medicaid members, undeliverables, and members without a phone number. A sample was not selected for the child members.
Among the 1000 adult members who were called, 488 (49%) had either wrong phone numbers or non–working numbers, 276 could not be reached after 5 telephone attempts, 25 did not speak English or Spanish, 96 refused, 8 were on extended vacations, 3 passed away, and 1 was incarcerated. A total of 103 surveys were completed.
This analysis supplements the non–respondent analysis above. The phone respondents are not true non–respondents, and the comparison between mail and phone respondents´ tests for differences between members who agree to participate in the mail survey with members who agree to participate in the phone survey.
Items from the mail survey that were included in the phone survey:
- How rate health of teeth and gums (Q1)
- How many times visited a dentist in the past 12 months (Q4)
- Whether have a regular dentist (Q9)
- Level of satisfaction with the overall quality of dental care received (Q13a)
Three additional questions were asked inquiring (a) whether members recalled receiving the mail surveys, (b) if so, why they did not complete and send back their surveys, and (c) whether members have a preference of survey mode (see Attachment #3 for phone survey).
The telephone survey findings were compared to the mail survey on demographic variables (i.e., gender, age, race/ethnicity, aid type) as well as responses to the four common questions. The mail and telephone respondents did not differ significantly on any of the demographic characteristics or the survey item responses. Note that these results should be interpreted with caution due to the fact that a small number of telephone respondents participated, and thus may not be representative of the general population. Among the 103 phone respondents, 25 said they received the survey, and 78 said they did not. When asked which mode they would be more likely to complete a survey in, 52 said by phone, 28 said by mail, and 13 said either by email or on the web. It makes sense that the number choosing phone is high since they did not complete the mail survey but agreed to do the phone survey.
Only 21 respondents replied to the question as to why they did not complete and return the survey. Five of these stated they did not have time, five stated they did return the survey (although there was no record that they actually did), and two stated they did not understand the survey items.
B. Descriptive Results of Enrollee Survey
This section consists of the raw frequencies for all items in the survey, categorized by domain for ease of evaluating the results. All results were itemized based on type of survey (adult MMC, adult FFS, child MMC, and child FFS). Attachment 4 displays the results for each respondent category. Below, results focus on the MMC group, combining adults and children.
Background Characteristics of Respondents
Table 6 displays the responses to the items comprising the background characteristics of the members. Age was not a survey item but was provided by the NYSDOH. Among the 1,255 adult respondents, age ranged from 18 to 65, with a mean of 40 years old. Among the 1,075 children, age ranged from 4 to 17, with a mean of 13 years old.
Among the combined age groups in the MMC cohort, 39% were male. A total of 72% had at least a high school diploma. Of the respondents, 33% were white, 33% black, 24% Hispanic, and 9% other.
Table 6. Background Characteristics
| Survey Item | MMC n * 1,816 |
||
|---|---|---|---|
| n | % | ||
| 16 | Gender (n = 1,719) | ||
| Male | 662 | 38.5 | |
| Female | 1057 | 61.5 | |
| 18 | Education (n = 1,667) | ||
| Less than H.S. | 463 | 27.8 | |
| High School | 844 | 50.6 | |
| College degree or more | 360 | 21.6 | |
| 19 | Race/ethnicity (n = 1,642) | ||
| White | 549 | 33.4 | |
| Black or African–American | 544 | 33.1 | |
| Hispanic or Latino | 397 | 24.2 | |
| Asian | 120 | 7.3 | |
| Native American (open–ended response) | 10 | 0.6 | |
| Arab (open–ended response) | 12 | 0.7 | |
| Mixed Race (open–ended response) | 10 | 0.6 | |
Oral Health Status
Responses to items pertaining to respondents´ dental health status are shown in Table 7. Regarding ratings of health of teeth and gums, members were almost equally distributed between favorable and unfavorable ratings. One–third reported that they had some major tooth or gum pain in the past 12 months.
Table 7. Oral Health Status
| Survey Item | MMC | ||
|---|---|---|---|
| n | % | ||
| 1 | Health of teeth/gums (n = 1,794) | ||
| Excellent | 199 | 11.1 | |
| Very good | 369 | 20.6 | |
| Good | 614 | 34.2 | |
| Fair | 406 | 22.6 | |
| Poor | 206 | 11.5 | |
| 2 | Had major tooth or gum pain in the past 12 months (n = 1,778) | ||
| Yes | 586 | 33.0 | |
| No | 1192 | 67.0 | |
Dental Care Information
The majority of members visited a dentist within the past year, while 47% reported going at least twice (see Table 8). Half of the respondents said they went to the dentist as often as needed within the past year. The major reason they last visited the dentist was for a regular check–up or cleaning (58%), while the remainder went for a tooth or gum problem, dentures, or braces. A total of 71% usually go to a private dental office for dental care, while 27% go to a health center, community clinic, or hospital outpatient department.
Two–thirds reported that they have a dentist that they see on a regular basis. Regarding dental care behaviors, 81% reported they brush their teeth at least twice a day, 55% visit a dentist at least twice a year, 61% have their teeth professionally cleaned at least once a year, and 40% floss regularly.
Table 8. Dental Care Information
| Survey Item | MMC | ||
|---|---|---|---|
| n | % | ||
| 3 | Last time visited a dentist (n = 1,799) | ||
| Less than 1 year ago | 1,143 | 63.5 | |
| Between 1 and 2 years ago | 340 | 18.9 | |
| Over 2 years ago | 238 | 13.2 | |
| Never | 78 | 4.3 | |
| 4 | Number of times visited a dentist in the past 12 months (n = 1,800) | ||
| 0 | 446 | 24.8 | |
| 1 time | 501 | 27.8 | |
| 2 times | 501 | 27.8 | |
| 3 or more times | 352 | 19.6 | |
| 5 | Whether went to the dentist as often as needed within the past 12 months (n = 1,785) | ||
| Yes | 900 | 50.4 | |
| No | 885 | 49.6 | |
| 6 | Reason visited dentist last time (n = 1,613) | ||
| Regular check–up / cleaning | 934 | 57.9 | |
| Tooth or gum problem | 627 | 38.9 | |
| Dentures (open–ended response) | 32 | 2.0 | |
| Braces (open–ended response) | 20 | 1.2 | |
| 8 | Where usually go for dental care (n = 1,664) | ||
| Health center / Community clinic / Hospital outpatient department | 442 | 26.6 | |
| Private dental office | 1180 | 70.9 | |
| Dental school | 18 | 1.1 | |
| Don´t go (open–ended response) | 24 | 1.4 | |
| 9 | Have a dentist to see on a regular basis (n = 1,730) | ||
| Yes | 1161 | 67.1 | |
| No | 569 | 32.9 | |
| 14a | Brush teeth at least 2 times a day (n = 1,739) | ||
| Yes | 1414 | 81.3 | |
| No | 325 | 18.7 | |
| 14b | Visit a dentist at least twice a year (n = 1,725) | ||
| Yes | 955 | 55.4 | |
| No | 770 | 44.6 | |
| 14c | Have teeth professionally cleaned at least once a year (n = 1,752) | ||
| Yes | 1061 | 60.6 | |
| No | 691 | 39.4 | |
| 14d | Use dental floss regularly (n = 1,716) | ||
| Yes | 685 | 39.9 | |
| No | 1031 | 60.1 | |
Barriers/Facilitators to Care
A total of 62% reported at least one difficulty in seeing a dentist as often as needed (see Table 9). The most common barriers cited were afraid or nervous to go (15%), dentists called do not accept their insurance (14%), do not like dentists or their particular dentists (13%), it is difficult to schedule an appointment (12%), have to wait too long in the waiting room (11%), and have trouble getting transportation (9%). Among the 95 open–ended responses, the most common difficulties cited were that Medicaid does not cover services they need, they do not have Medicaid, insurance, or a card, the office location is not convenient, and Medicaid dentists are not good. Most members reported that their health plan has a dental benefit (84%).
When asked what would help them see the dentist more often, 78% cited at least one facilitator. The most common were more dentists to choose from (32%), reminders to visit the dentist (31%), better communication about benefits from their health plan (24%), and more convenient office hours (18%). Among the 112 open–ended responses, the most common facilitators cited were that they want more specific dental benefits covered, closer location, and better dentists to choose from.
Table 9. Barriers/Facilitators to Care
| Survey Item | MMC | ||
|---|---|---|---|
| n | % | ||
| 7@ | Major difficulties had in seeing a dentist as often as needed (n = 1,680) | ||
| Have not had difficulty in seeing a dentist | 646 | 38.5 | |
| Afraid or nervous to go | 255 | 15.2 | |
| The dentists I called do not accept my insurance | 234 | 13.9 | |
| Do not like my dentist / dentists in general | 218 | 13.0 | |
| It is difficult to schedule an appt. | 196 | 11.7 | |
| Have to wait too long in the waiting room | 183 | 10.9 | |
| Have trouble getting transportation | 151 | 9.0 | |
| Forget to go | 133 | 7.9 | |
| Have trouble getting orthodontic care | 114 | 6.8 | |
| Dentist does not have convenient office hours | 99 | 5.9 | |
| Medicaid does not cover dentists | 88 | 5.2 | |
| Have trouble finding a dentist who speaks my language | 84 | 5.0 | |
| Don´t know how to find a dentist | 83 | 4.9 | |
| Can´t take time off from work | 76 | 4.5 | |
| Don´t have time | 74 | 4.4 | |
| Don´t have someone to watch children | 52 | 3.1 | |
| Cannot find office with handicap accessibility | 9 | 0.5 | |
| Other (open–ended responses): | 95 | 5.7 | |
| Medicaid does not cover services I need | 32 | ||
| Do not have Medicaid / insurance / card | 13 | ||
| Office location not convenient | 11 | ||
| Medicaid dentists are not good | 11 | ||
| Expense / out–of–pocket costs | 7 | ||
| Unclean office | 5 | ||
| Not enough choices of dentists in Medicaid | 5 | ||
| Other medical problems | 2 | ||
| Have no teeth | 1 | ||
| Other | 8 | ||
| 14e | My health plan has a dental benefit (n = 1,664) | ||
| Yes | 1391 | 83.6 | |
| No | 273 | 16.4 | |
| 15@ | What would help see the dentist more often (n = 1,669) | ||
| None. I see the dentists as often as I like. | 363 | 21.7 | |
| More dentists to choose from | 527 | 31.6 | |
| Reminders to visit dentist | 513 | 30.7 | |
| Better communication about benefits from my health plan | 405 | 24.3 | |
| More convenient office hours | 298 | 17.9 | |
| Education about good dental care | 256 | 15.3 | |
| Help with transportation to the dentist | 253 | 15.2 | |
| Dentists that speak my language | 248 | 14.9 | |
| Help in finding a dentist | 248 | 14.9 | |
| Other (open–ended responses): | 112 | 6.7 | |
| Want more specific dental benefits covered | 44 | ||
| Closer location | 15 | ||
| Better dentists to choose from | 14 | ||
| Help with anxiety | 11 | ||
| Faster appointment times | 8 | ||
| Better price | 5 | ||
| Equal treatment for Medicaid patients | 4 | ||
| Faster approval from Medicaid | 4 | ||
| Less waiting time at dental office | 2 | ||
| I have no teeth / have dentures | 2 | ||
| Handicap accessible | 1 | ||
| Other | 2 | ||
@ Multiple responses
Access and Availability of Dental Care
Three questions evaluated the ability of members to locate care and the ease of obtaining timely care (see Table 10). Each of these questions is based on members who have a regular dentist. Most members found their dentist based on the provider directory from their plan (45%) or a referral from a family member or friend (34%).
When asked how long they usually have to wait for an appointment if they have a dental problem, 29% stated they never needed a dentist for emergency care. After excluding those members who did not need a dentist, 35% reported they had to wait less than a day, 27% reported 1 to 2 days wait, 24% reported 3 days to 1 week, and 14% reported longer than 1 week. The usual wait for an appointment for a regular check–up was less than 1 month for 74% of the respondents, 1 to 3 months for 21%, and longer than 3 months for 5%.
Table 10. Access and Availability of Dental Care
| Survey Item | MMC | ||
|---|---|---|---|
| n | % | ||
| 10@ ◆ |
How found dentist (n = 1,114) | ||
| Provider directory from plan | 502 | 45.1 | |
| Referral from family / friend | 380 | 34.1 | |
| Referral from a PCP / doctor / nurse | 202 | 18.1 | |
| Telephone book | 47 | 4.2 | |
| Advertisement / Flyer | 39 | 3.5 | |
| Other (open–ended responses): In local neighborhood, walk–in Using long–term dentist Other |
35 24 8 3 |
3.1 | |
| 11 ◆ | How long usually have to wait for an appt. if have a dental problem (n = 1,140) | ||
| Less than 1 day | 281 | 24.6 | |
| 1 to 2 days | 222 | 19.5 | |
| 3 days to 1 week | 195 | 17.1 | |
| Longer than 1 week | 115 | 10.1 | |
| Never needed a dentist for emergency care EB | 327 | 28.7 | |
| 12 ◆ | How long usually have to wait for an appt. if want a regular check–up (n = 1,130) | ||
| Less than 1 month | 835 | 73.9 | |
| 1 to 3 months | 235 | 20.8 | |
| Longer than 3 months | 60 | 5.3 | |
@ Multiple responses
◆ Items based on skip pattern; rates based on respondents with a regular dentist.
⊕ Note: this response category is only presented here, and is excluded from other analyses.
Satisfaction with Dental Care and Health Plan
Among members who have a regular dentist, ratings of "very satisfied" ranged from 43% for wait to get an appointment to 63% for cleanliness of the office (see Table 11). Ratings of dissatisfaction (either somewhat or very) ranged from 9% for office cleanliness to 18% for wait to get an appointment.
Ratings of health plans were lower than ratings of dental care. Satisfaction with health plans´ explanation of dental benefits was distributed as 56% satisfied, 21% neutral, and 24% dissatisfied. Regarding the number of dentists to choose from, 47% were satisfied, 22% were neutral, and 31% were dissatisfied.
Table 11. Satisfaction with Dental Care and Health Plan
| Survey Item | MMC | ||
|---|---|---|---|
| n | % | ||
| 13a ◆ |
Satisfaction with overall quality of dental care received (n = 1,087) | ||
| Very satisfied | 541 | 49.8 | |
| Somewhat satisfied | 266 | 24.5 | |
| Neutral | 158 | 14.5 | |
| Somewhat dissatisfied | 60 | 5.5 | |
| Very dissatisfied | 62 | 5.7 | |
| 13a ◆ |
Satisfaction with dental advice received (n = 1,064) | ||
| Very satisfied | 522 | 49.1 | |
| Somewhat satisfied | 268 | 25.2 | |
| Neutral | 151 | 14.2 | |
| Somewhat dissatisfied | 66 | 6.2 | |
| Very dissatisfied | 57 | 5.4 | |
| 13a ◆ |
Satisfaction with cleanliness of the office (n = 1,083) | ||
| Very satisfied | 677 | 62.5 | |
| Somewhat satisfied | 209 | 19.3 | |
| Neutral | 103 | 9.5 | |
| Somewhat dissatisfied | 44 | 4.1 | |
| Very dissatisfied | 50 | 4.6 | |
| 13a ◆ |
Satisfaction with friendliness/helpfulness of staff (n = 1,099) | ||
| Very satisfied | 655 | 59.6 | |
| Somewhat satisfied | 230 | 20.9 | |
| Neutral | 109 | 9.9 | |
| Somewhat dissatisfied | 49 | 4.5 | |
| Very dissatisfied | 56 | 5.1 | |
| 13a ◆ |
Satisfaction with convenience of location (n = 1,069) | ||
| Very satisfied | 643 | 60.1 | |
| Somewhat satisfied | 215 | 20.1 | |
| Neutral | 96 | 9.0 | |
| Somewhat dissatisfied | 48 | 4.5 | |
| Very dissatisfied | 67 | 6.3 | |
| 13a ◆ |
Satisfaction with office hours (n = 1,054) | ||
| Very satisfied | 530 | 50.3 | |
| Somewhat satisfied | 284 | 26.9 | |
| Neutral | 112 | 10.6 | |
| Somewhat dissatisfied | 65 | 6.2 | |
| Very dissatisfied | 63 | 6.0 | |
| 13a ◆ |
Satisfaction with wait to get an appointment (n = 1,056) | ||
| Very satisfied | 455 | 43.1 | |
| Somewhat satisfied | 268 | 25.4 | |
| Neutral | 139 | 13.2 | |
| Somewhat dissatisfied | 102 | 9.7 | |
| Very dissatisfied | 92 | 8.7 | |
| 13b | Satisfaction with health plan´s explanation of dental benefits (n = 1,573) | ||
| Very satisfied | 520 | 33.1 | |
| Somewhat satisfied | 355 | 22.6 | |
| Neutral | 325 | 20.7 | |
| Somewhat dissatisfied | 162 | 10.3 | |
| Very dissatisfied | 211 | 13.4 | |
| 13b | Satisfaction with number of dentists to choose from (n = 1,507) | ||
| Very satisfied | 409 | 27.1 | |
| Somewhat satisfied | 296 | 19.6 | |
| Neutral | 329 | 21.8 | |
| Somewhat dissatisfied | 179 | 11.9 | |
| Very dissatisfied | 294 | 19.5 | |
◆ Items based on skip pattern; rates based on respondents with a regular dentist.
C. Comparisons of Age Groups on All Enrollee Survey Items
To assess whether differences exist between children and adults, group comparisons were performed on each of the survey items. Unlike the frequency distributions in Section B, items that contained many response options were re–coded into fewer categories for chi–square analyses. These analyses were limited to the MMC cohort.
Table 12 displays the results. Statistically significant differences emerged on race/ethnicity, oral health status, many of the dental care indicators, barriers and facilitators to care, and two of the nine satisfaction items. Children were more likely to be Hispanic than adults. Children were more likely to have good oral health status, to receive appropriate dental care visits, and to be satisfied with care, and less likely to report barriers or facilitators to care than adults. No differences were found on the access and availability indicators.
Table 12. Comparison of Children and Adults
| Survey Item | Adults n = 952 |
Children n = 864 |
p value | |
|---|---|---|---|---|
| Background Characteristics of Respondents | ||||
| 19 | Race/ethnicity | 0.0001 | ||
| White | 34.6% | 32.1% | ||
| Black or African–American | 36.7% | 29.1% | ||
| Hispanic or Latino | 20.3% | 28.6% | ||
| Other | 8.5% | 10.1% | ||
| Oral Health Status | ||||
| 1 | Health of teeth/gums is excellent, very good, or good | 53.5% | 79.5% | 0.0001 |
| 2 | Had major tooth or gum pain in the past 12 months | 44.0% | 21.0% | 0.0001 |
| Dental Care Information | ||||
| 3 | Visited a dentist < 1 year ago | 57.2% | 70.5% | 0.0001 |
| 4 | Visited a dentist 1+ times in the past 12 months | 70.9% | 80.0% | 0.0001 |
| 5 | Went to the dentist as often as needed within the past 12 months | 39.1% | 62.8% | 0.0001 |
| 6 | Visited dentist last time for regular check–up / cleaning | 42.6% | 74.6% | 0.0001 |
| 8 | Usually get dental care at private office | 74.2% | 69.5% | n.s. |
| 9 | Have a dentist to see on a regular basis | 59.0% | 76.0% | 0.0001 |
| 14a | Brush teeth at least 2 times a day | 83.3% | 79.2% | n.s. |
| 14b | Visit a dentist at least 2 times a year | 47.5% | 63.6% | 0.0001 |
| 14c | Have teeth professionally cleaned 1+ a year | 51.6% | 70.3% | 0.0001 |
| 14d | Use dental floss regularly | 45.6% | 33.9% | 0.0001 |
| Barriers/Facilitators to Care | ||||
| 7 | No major difficulties in seeing a dentist as often as needed | 30.8% | 47.0% | 0.0001 |
| 14e | My health plan has a dental benefit | 79.7% | 87.8% | 0.0001 |
| 15 | Nothing would help me see the dentist more often | 17.1% | 26.9% | 0.0001 |
| Access and Availability of Dental Care | ||||
| 10 @ ◆ |
How found dentist | |||
| Referral from family / friend | 36.8% | 31.8% | n.s. | |
| Referral from a PCP / doctor / nurse | 16.8% | 19.3% | n.s. | |
| Provider directory from plan | 41.6% | 48.1% | n.s. | |
| Other | 11.8% | 9.2% | n.s. | |
| 11 ◆ | Usually wait < 1 day for an appt. for dental problem | 32.7% | 36.3% | n.s. |
| 12 ◆ | Usually wait < 1 month for an appt. for regular check–up | 73.9% | 73.9% | n.s. |
| Very / Somewhat Satisfied with: | ||||
| 13a ◆ |
Overall quality of dental care received | 71.2% | 76.7% | n.s. |
| Dental advice received | 69.2% | 78.2% | 0.001 | |
| Cleanliness of the office | 81.4% | 82.1% | n.s. | |
| Friendliness/helpfulness of staff | 80.7% | 80.4% | n.s. | |
| Convenience of location | 83.0% | 78.1% | n.s. | |
| Office hours | 76.8% | 77.6% | n.s. | |
| Wait to get an appointment | 71.4% | 66.1% | n.s. | |
| 13b | Health plan´s explanation of dental benefits | 48.4% | 63.0% | 0.0001 |
| Number of dentists to choose from | 43.2% | 50.5% | n.s. | |
Note: Bold values represent the statistically higher value in that row.
@ Multiple responses
◆ Items based on skip pattern; rates based on respondents with a regular dentist.
D. Predictors of Responses to Selected Survey Items
Multivariate analyses were performed to identify predictors of dental visits, problems with receipt of care, and satisfaction with care. These analyses determined whether the group comparisons on the survey items are statistically significant after controlling for potentially confounding characteristics. This section was limited to the MMC cohort.
Five logistic regressions were performed, one for each dependent variable, across several domains:
Dental care information
- Whether visited a dentist in the past 12 months (Q4)
Barriers/Access
- Whether experienced difficulties in seeing a dentist as often as needed (Q7)
- Length of time to wait for an appointment for a regular check–up (Q12)
Satisfaction
- Whether satisfied with the overall quality of dental care received (Q13a)
- Whether satisfied with the number of dentists to choose from health plan (Q13b)
The following eight variables served as independent variables in each of the regressions:
- Age group (adult vs. child)
- Gender – item 16 (male vs. female)
- Race/ethnicity – item 19 (3 dummy variables: white vs. all others; black vs. all others; Hispanic vs. all others)
- Education – item 18 (less than high school vs. at least high school)
- NY region (NYC vs. Rest of state)
- Whether have a regular dentist – item 9 (yes vs. no)
- Usual place for dental care – item 8 (private office vs. clinic / outpatient department / dental school)
- Health status of teeth and gums – item 1 (excellent / very good / good vs. fair / poor)
For each of the dependent variables, Table 13 lists the variables with significant associations (with a p value of .001) via the multivariate regressions after controlling for potential confounding effects.
As can be seen, few significant relationships were detected, although each item was related to at least one of the eight predictors. The two most common significant predictors were whether the member has a regular dentist and the health of the member´s teeth and gums.
Dental care information
For "whether visited a dentist in the past 12 months", having a regular dentist was the only significant variable. Members who have a regular dentist were more likely to report that they have visited a dentist in the past 12 months than were members who do not have a regular dentist.
Barriers/Access
For "whether experienced difficulties in seeing a dentist as often as needed", two variables were significant. Members who have a regular dentist and members who rated the health of their teeth/gums positively were more likely to say they have no difficulties than their counterparts (i.e., members who do not have a regular dentist and members who rated their teeth/gums negatively, respectively). Conversely, members without a regular dentist and members who rated the health of their teeth/gums negatively were more likely to report at least one difficulty in seeing a dentist.
For "length of time to wait for an appointment for a regular check–up", three variables were significant. Members who were black, those who resided in NYC, and those whose usual place of care is at a private dental office were more likely to report that they receive an appointment within one month than their counterparts (i.e., members who were not black, those who resided outside of NYC, and those whose usual place of care is at a health center, community clinic, hospital outpatient department, or dental school, respectively).
Satisfaction
Only one variable was significantly related to "satisfaction with the overall quality of dental care received". Members who rated the health of their teeth/gums positively were more likely to be satisfied than those who rated the health negatively.
For "satisfaction with the number of dentists to choose from the health plan", three variables emerged as statistically significant. Members who were black, those with a regular dentist, and those who rated their teeth/gums positively were more likely to be satisfied than their counterparts (i.e., those who were not black, those without a regular dentist, and those who rated their teeth/gums negatively, respectively).
Table 13. Significant Associations with Logistic Regression
| Survey Item | N | Statistically Significant Variables (p < .001) |
|
|---|---|---|---|
| 4 | Whether visited a dentist in the past 12 months | 1368 | Have a Regular Dentist |
| 7 | Whether experienced difficulties in seeing a dentist as often as needed | 1295 | Have a Regular Dentist Health of Teeth/Gums |
| 12 ◆ | Length of time to wait for an appointment for a regular check–up | 955 | Race = Black NY Region Usual Place of Care |
| 13a ◆ | Satisfaction with the overall quality of dental care received | 918 | Health of Teeth/Gums |
| 13b | Satisfaction with number of dentists to choose from health plan | 1170 | Race = Black Have a Regular Dentist Health of Teeth/Gums |
◆ Items based on skip pattern; rates based on respondents with a regular dentist.
E. MCO Variation
To examine variation among plans on each of the survey items, the minimum rate, maximum rate, range, and median rate performance among plans are displayed for each survey item in Table 14. The analysis was based on the 16 MMC plans. Both children and adults were combined for the analysis. Across the 16 plans, the number of respondents ranged from 69 to 146, with a total of 1,816 respondents. The actual number of cases varied for each item, but each plan survey item rate comprised at least 30 respondents. Whereas all other analyses presented in this report are based on individual members, the analyses presented in Table 14 are based on individual plans, and thus, depict plan performance.
Based on the range, the diversity in plan rate variation differs among the items. Items with the widest range included:
- race/ethnicity,
- whether usually receive dental care at a private office, and
- how members found their dentist (e.g., referral from friend/family or provider directory).
Moderate variation was found for:
- how long members have to wait to get an appointment for a dental problem or for a regular checkup and for
- several of the satisfaction items.
Relatively small variation among plans was detected for:
- oral health status and
- some of the dental care indicators, such as whether visit a dentist at least twice a year and whether have teeth professionally cleaned at least once a year.
Note that prior to performing this analysis, IPRO evaluated the potential need for risk– adjusting the rates on the survey items when reporting MCO–specific rates. Specifically, 3 separate sets of regressions (Adult, Children, and Long–term Care) were conducted to determine whether various demographic variables (race/ethnicity, gender, NY region, age group, and aid type category) were related to each of the 29 survey items (resulting in 87 regressions). Very few variables yielded significance. Hence, risk–adjustment was deemed unnecessary and the raw MCO–specific rates were presented.
In addition, MCO–specific results are provided as one–page summaries in a separate document, including survey responses for each MCO as well as statewide averages.
Table 14. MCO Variability
| Survey Item | Min | Max | Range | Median | |
|---|---|---|---|---|---|
| Background Characteristics of Respondents | |||||
| 16 | Male gender | 18% | 53% | 34% | 38% |
| 18 | High school graduate | 53% | 83% | 31% | 75% |
| 19 | Race/ethnicity | ||||
| White | 0% | 72% | 72% | 27% | |
| Black or African–American | 11% | 69% | 58% | 30% | |
| Hispanic or Latino | 3% | 79% | 76% | 21% | |
| Other | 1% | 29% | 28% | 4% | |
| Oral Health Status | |||||
| 1 | Health of teeth/gums is excellent, very good, or good | 54% | 74% | 20% | 66% |
| 2 | Had major tooth or gum pain in the past 12 months | 26% | 42% | 16% | 33% |
| Dental Care Information | |||||
| 3 | Visited a dentist < 1 year ago | 52% | 76% | 24% | 63% |
| 4 | Visited a dentist 1+ times in the past 12 months | 65% | 84% | 19% | 74% |
| 5 | Went to the dentist as often as needed within the past 12 months | 38% | 63% | 26% | 50% |
| 6 | Visited dentist last time for regular check–up / cleaning | 48% | 68% | 20% | 57% |
| 8 | Usually get dental care at private office | 16% | 91% | 75% | 78% |
| 9 | Have a dentist to see on a regular basis | 56% | 79% | 23% | 67% |
| 14a | Brush teeth at least 2 times a day | 72% | 93% | 21% | 81% |
| 14b | Visit a dentist at least 2 times a year | 49% | 66% | 17% | 55% |
| 14c | Have teeth professionally cleaned 1+ a year | 53% | 69% | 16% | 60% |
| 14d | Use dental floss regularly | 33% | 52% | 18% | 41% |
| Barriers/Facilitators to Care | |||||
| 7 | No major difficulties in seeing a dentist as often as needed | 25% | 53% | 28% | 39% |
| 14e | My health plan has a dental benefit | 76% | 93% | 17% | 83% |
| 15 | Nothing would help me see the dentist more often | 14% | 29% | 16% | 21% |
| Access and Availability of Dental Care | |||||
| 10@ ◆ | How found dentist | ||||
| Referral from family / friend | 11% | 64% | 53% | 27% | |
| Referral from a PCP / doctor / nurse | 11% | 38% | 28% | 18% | |
| Provider directory from plan | 20% | 66% | 46% | 47% | |
| Other | 3% | 18% | 14% | 11% | |
| 11 ◆ | Usually wait < 1 day for an appt. for dental problem | 12% | 45% | 33% | 34% |
| 12 ◆ | Usually wait < 1 month for an appt. for regular check–up | 55% | 91% | 36% | 72% |
| Very / Somewhat Satisfied with: | |||||
| 13a ◆ | Overall quality of dental care received | 58% | 83% | 25% | 76% |
| Dental advice received | 52% | 84% | 32% | 76% | |
| Cleanliness of the office | 64% | 88% | 24% | 82% | |
| Friendliness/helpfulness of staff | 50% | 88% | 38% | 82% | |
| Convenience of location | 66% | 89% | 23% | 81% | |
| Office hours | 55% | 87% | 31% | 77% | |
| Wait to get an appointment | 41% | 79% | 38% | 70% | |
| 13b | Health plan´s explanation of dental benefits | 43% | 64% | 20% | 57% |
| Number of dentists to choose from | 27% | 56% | 29% | 48% | |
@ Multiple responses
◆ Items based on skip pattern; rates based on respondents with a regular dentist.
F. Comparisons of Vendor Utilization on Enrollee Survey Items
Plans that used a dental vendor in 2005 were compared with plans that did not to determine whether any differences existed on the survey responses. Twelve plans with 1,297 respondents represented the former group and four plans (i.e., Americhoice, CarePlus, Community Choice, and St. Barnabas) with 519 respondents represented the latter group. Table A–1 in Attachment 5 presents the results. These analyses were limited to the MMC cohort, and combined children and adults.
Because the groups differed significantly on race/ethnicity, crosstabulations were verified by performing a logistic regression on each survey item as a dependent variable, and including vendor as an independent variable, after controlling for race/ethnicity. Items # 8 and 10 were the only significant variables via both chi–square and the regressions. Members from plans using a vendor were more likely to get care at a private dental office (75%) compared to members not using a vendor (64%). Those with a vendor were also more likely to have found a dentist via their provider directory and less likely to have used a referral from a family or friend compared to those without a vendor.
In addition, among the subset of 12 plans that use a vendor, comparisons were made on each survey item comparing the sets of plans with different dental vendors (see Table A–2 in Attachment 5 for results). Five plans used Doral (i.e., Fidelis, GHI HMO, HealthFirst, Managed Health, and NY Hospital) and seven plans used HealthPlex (Affinity, Health Plus, HIP, Hudson, MVP, Neighborhood, and United).
Members from plans that used Doral (n = 532) were compared to members from plans that used HealthPlex (n = 765). Only two items were identified with statistically significant differences between the groups. Members of plans that use the Doral vendor were more likely to find their dentist using referrals from family and friends, whereas members of plans that use the HealthPlex vendor were more likely to find their dentist via the provider directory.
G. Comparisons of MMC and FFS Medicaid Groups
To investigate differences between responses for the managed care cohort and the FFS Medicaid cohort, comparisons were performed on each of the survey items. Table 15 displays the results. Because the groups differed significantly on race/ethnicity, crosstabulations were verified by performing a logistic regression on each survey item as a dependent variable, and including payor as an independent variable, after controlling for race/ethnicity. Results across the statistical analyses were consistent.
Several statistically significant differences were identified between the FFS Medicaid and MMC cohorts. The MMC cohort was more likely to be black and less likely to be white compared to the FFS cohort. Compared to the FFS cohort, the MMC cohort was more likely to report good oral health status, that they last visited a dentist less than a year ago, that they visited a dentist at least once in the past year, that they usually go to a private dentist office, and that they usually wait less than one month for an appointment for a regular check–up. The FFS Medicaid cohort was more likely to report that they choose their dentist based on recommendations from family or friends. No differences appeared on barriers/facilitators to dental care or satisfaction with care.
Table 15. Comparison of MMC versus FFS Medicaid
| Survey Item | FFS | MMC | p value | ||||
|---|---|---|---|---|---|---|---|
| n = 514 | n = 1,816 | ||||||
| Background Characteristics of Respondents | |||||||
| 16 | Male gender | 36.3% | 38.5% | n.s. | |||
| 18 | High school graduate | 68.3% | 72.2% | n.s. | |||
| 19 | Race/ethnicity | 0.0001 | |||||
| White | 50.3% | 33.4% | |||||
| Black or African–American | 20.8% | 33.1% | |||||
| Hispanic or Latino | 21.6% | 24.2% | |||||
| Other | 7.3% | 9.3% | |||||
| Oral Health Status | |||||||
| 1 | Health of teeth/gums is excellent, very good, or good | 57.4% | 65.9% | 0.0001 | |||
| 2 | Had major tooth or gum pain in the past 12 months | 37.9% | 33.0% | n.s. | |||
| Dental Care Information | |||||||
| 3 | Visited a dentist < 1 year ago | 54.8% | 63.5% | 0.0001 | |||
| 4 | Visited a dentist 1+ times in the past 12 months | 63.4% | 75.2% | 0.0001 | |||
| 5 | Went to the dentist as often as needed within the past 12 months | 46.6% | 50.4% | n.s. | |||
| 6 | Visited dentist last time for regular check–up / cleaning | 54.6% | 57.9% | n.s. | |||
| 8 | Usually get dental care at private office | 52.4% | 72.0% | 0.0001 | |||
| 9 | Have a dentist to see on a regular basis | 61.1% | 67.1% | n.s. | |||
| 14a | Brush teeth at least 2 times a day | 75.2% | 81.3% | n.s. | |||
| 14b | Visit a dentist at least 2 times a year | 49.5% | 55.4% | n.s. | |||
| 14c | Have teeth professionally cleaned 1+ a year | 53.0% | 60.6% | n.s. | |||
| 14d | Use dental floss regularly | 41.3% | 39.9% | n.s. | |||
| Barriers/Facilitators to Care | |||||||
| 7 | No major difficulties in seeing a dentist as often as needed | 35.5% | 38.5% | n.s. | |||
| 14e | My health plan has a dental benefit | 78.0% | 83.6% | n.s. | |||
| 15 | Nothing would help me see the dentist more often | 20.2% | 21.7% | n.s. | |||
| Access and Availability of Dental Care | |||||||
| 10 @ ◆ |
How found dentist | ||||||
| Referral from family / friend | 48.4% | 34.1% | 0.0001 | ||||
| Referral from a PCP / doctor / nurse | 19.6% | 18.1% | n.s. | ||||
| Provider directory from plan | 20.3% | 45.1% | 0.0001 | ||||
| Other | 22.4% | 10.4% | 0.0001 | ||||
| 11 ◆ | Usually wait < 1 day for an appt. for dental problem | 32.5% | 34.6% | n.s. | |||
| 12 ◆ | Usually wait < 1 month for an appt. for regular check–up | 61.2% | 73.9% | 0.0001 | |||
| Very / Somewhat Satisfied with: | |||||||
| 13a ◆ |
Overall quality of dental care received | 75.4% | 74.2% | n.s. | |||
| Dental advice received | 74.0% | 74.2% | n.s. | ||||
| Cleanliness of the office | 86.0% | 81.8% | n.s. | ||||
| Friendliness/helpfulness of staff | 87.3% | 80.5% | n.s. | ||||
| Convenience of location | 79.9% | 80.3% | n.s. | ||||
| Office hours | 81.3% | 77.2% | n.s. | ||||
| Wait to get an appointment | 68.1% | 68.5% | n.s. | ||||
| 13b | Health plan´s explanation of dental benefits | 52.6% | 55.6% | n.s. | |||
| Number of dentists to choose from | 40.4% | 46.8% | n.s. | ||||
Note: Bold values represent the statistically higher value in that row.
@ Multiple responses
◆ Items based on skip pattern; rates based on respondents with a regular dentist.
H. Other Analyses
Racial Disparities in Barriers and Facilitators
Additional analyses were performed to identify any racial disparities in barriers or facilitators to dental care. The analyses were limited to the MMC cohort. Race was dichotomized as white or other (including black, Hispanic, and other). The two groups were compared on each of the response options to items #7 (difficulties in seeing a dentist as often as needed) and #15 (what would help see the dentist more). Fisher´s exact test was computed when in a few instances one or more cells in the cross tabulation had an expected frequency of less than 5.
Table 16 displays the results. Compared to whites, other races were more likely to report that their major barriers to care were that they forget to go and have trouble finding a dentist who speaks their language. In contrast, whites were more likely to report that the dentists they called do not accept their insurance.
Similar results were revealed in comparing the groups on facilitators to care. The other races were more likely to report that reminders to visit the dentist, dentists that speak their language, and education about good dental care would help them see the dentist, while whites were more likely to report that more dentists to choose from would help them see a dentist more often. No significant differences between the racial groups appeared on the remaining barriers and facilitators.
Differences between FFS Medicaid and MMC on Barriers and Facilitators
The 2 payor groups, FFS Medicaid and MMC, were also compared on each of the individual barriers and facilitators (table not shown). Members comprising the FFS cohort (n = 514) differed from members comprising the MMC cohort (n = 1,816) on only one barrier. The FFS members (14%) were more likely to report transportation as a major difficulty in seeing the dentist than the MMC members (9%). No differences appeared on facilitators.
Table 16. Comparison of Whites and Other Races
| Survey Item | Whites n = 549 |
Other n = 1,093 |
p value | |
|---|---|---|---|---|
| Barriers to Care | ||||
| Have not had difficulty in seeing a dentist | 37.6% | 39.1% | n.s. | |
| Have trouble getting transportation | 9.1% | 8.5% | n.s. | |
| Forget to go | 4.6% | 10.0% | 0.0001 | |
| Do not like my dentist / dentists in general | 14.6% | 11.8% | n.s. | |
| It is difficult to schedule an appt. | 12.7% | 11.3% | n.s. | |
| Dentist does not have convenient office hours | 6.6% | 5.4% | n.s. | |
| Have to wait too long in the waiting room | 10.6% | 11.3% | n.s. | |
| Afraid or nervous to go | 16.6% | 15.2% | n.s. | |
| Don´t have time | 4.8% | 4.5% | n.s. | |
| Don´t have someone to watch children | 4.2% | 2.3% | n.s. | |
| Can´t take time off from work | 5.0% | 4.6% | n.s. | |
| Don´t know how to find a dentist | 6.2% | 4.7% | n.s. | |
| Cannot find office with handicap accessibility | 0.2% | 0.7% | n.s. | |
| Have trouble finding a dentist who speaks my language | 1.3% | 6.7% | 0.0001 | |
| Have trouble getting orthodontic care | 6.0% | 7.5% | n.s. | |
| The dentists I called do not accept my insurance | 21.6% | 9.7% | 0.0001 | |
| Medicaid does not cover dentists | 6.9% | 4.3% | n.s. | |
| Facilitators to Care | ||||
| None. I see the dentists as often as I like. | 22.2% | 21.0% | n.s. | |
| Help with transportation to the dentist | 13.2% | 15.4% | n.s. | |
| Reminders to visit dentist | 24.2% | 34.5% | 0.0001 | |
| More dentists to choose from | 38.7% | 27.7% | 0.0001 | |
| More convenient office hours | 16.1% | 18.7% | n.s. | |
| Dentists that speak my language | 9.1% | 18.6% | 0.0001 | |
| Help in finding a dentist | 17.6% | 13.6% | n.s. | |
| Better communication about benefits from my health plan | 22.8% | 25.5% | n.s. | |
| Education about good dental care | 8.3% | 19.2% | 0.0001 | |
Note: Bold values represent the statistically higher value in that row.
|top of section| |top of page|DISCUSSION
Oral health is a central but often neglected component of general physical health. Although significant improvement has been achieved in the oral health of Americans over the past few decades, there remains opportunity for improvement, and disparities and gaps in access to dental care between lower income and higher income populations persist.1 Regular professional dental care is essential for maintaining oral health through prevention, early diagnosis and treatment of problems and assessment of appropriate home care.3
Access to dental services for lower income populations is problematic: those with incomes at or above the poverty level are twice as likely to report a dental visit in the past 12 months as those who are below the poverty level.2 Enrollment in Medicaid alone does not eliminate disparities between poor and non–poor children4.
This dental care study was undertaken to assess the apparent discrepancy between reported QARR rates for Annual Dental Visits and results of the Access and Availability survey, and to describe the dental care experience of New York State Medicaid MCO members, their satisfaction with the dental care they received, and their perceived barriers to accessing dental care. Survey respondents´ self–reported annual visit rates were markedly higher than 2004 New York State QARR rates, but barriers to care were cited, and opportunities for improvement exist, especially in the adult population.
Oral Health Status
Despite national improvement in oral health, millions of children and adults continue to experience dental caries and periodontal disease3. The survey respondents´ oral health was good or better for the majority, but one in three reported only fair or poor oral health and major problems in the past 12 months. Dental caries remains the most common chronic disease of childhood, and 34% of poor children nationally are reported to have one or more untreated decayed primary teeth compared to 13% of non–poor children12. When survey responses were stratified by adult/child respondents, oral health status was rated significantly better for children than adults, as would be expected, with 80% of children reported to have good or better health of teeth and gums versus only 54% of adults. One in five children were, however, reported to have had a major tooth or gum problem in the past 12 months. A total of 44% of adults reported major problems in the past year. Oral health status could potentially be improved with interventions that impact oral care behaviors and access to professional care.
Dental Care
Dental care behaviors for overall respondents present an opportunity for improvement; respondents reported an 81% rate of brushing teeth at least twice a day, while only 40% reported using dental floss regularly. Children were statistically less likely to use dental floss regularly (34%) than adults (46%). The American Academy of Pediatrics (AAP) recommends anticipatory guidance to include twice daily brushing for children as soon as teeth erupt and flossing daily; incorporating such guidance into primary care visits could assist in improving rates.5
Gaps in use of dental care services persist between low income and higher income populations in the United States, with poor children having significantly fewer preventive dental visits than those with higher incomes2. Even with Medicaid dental coverage, children enrolled in Medicaid nationally were reported to have low rates of preventive dental services in a given year1. Although survey respondents´ most commonly reported reason for the last dental visit was regular checkup or cleaning, only 61% of respondents report having teeth professionally cleaned at least once a year, with higher rates for children (70%) than adults (52%). Twice yearly regular dental visits were reported at rates of only 55% (64% for children and 48% for adults). Respondents cited education about good dental care as a potential facilitator to care. Although education and parental counseling regarding need for such preventive dental service can be helpful, the barriers to accessing such care are likely multifactorial and require more than one intervention to achieve improvement.
2004 HEDIS annual dental visit rates ranged from 10.5% to 53.0%. Of MMC members who completed the mailed survey, 75% of respondents visited a dentist one or more times in the past twelve months, with 47% visiting at least twice. Again, children fared better than the adult cohort, with statistically higher rates for dental visits within the past year for children (80% for children versus 71% for adults). The higher rates of annual visits reported by the surveyed population as compared to 2004 reported HEDIS rates could be affected by survey limitations such as response bias, as individuals who visited a dentist may have been more likely to complete the survey.
Barriers / Facilitators
Despite higher reported rates of annual visits than were reported in 2004 HEDIS, half of the respondents indicated that they did not see the dentist as often as needed. This unmet need was more pronounced in adults. Overall, 67% of respondent´s overall report having a dentist that they see regularly, but 76% of children report having a regular dentist. Having a regular dentist was the single significant variable for having visited a dentist in the past twelve months, with members who have a regular dentist more likely to have visited a dentist in the past twelve months, as well as to report no difficulties in seeing a dentist, than those without a regular dentist. The role of pediatric primary care providers in dental screening and referral has positively impacted access to dental care6. In its policy statement on oral health and the dental home, the American Academy of Pediatrics promotes the establishment of a dental home, a specialized primary dental care provider within the conceptual framework of the medical home, as an ideal approach to early childhood caries prevention5. Recommendations also include oral health risk assessments by pediatric health professionals, and anticipatory guidance and intervention by a dentist for those at risk, including children in families of low socioeconomic status. Inclusion of preventive dental services in EPSDT* screening likely positively impacts attention to oral health. Attention to oral health by adult primary care providers, with education and referral, could potentially increase access to preventive dental services by adults. Many respondents (31%) indicated reminders could facilitate care; such reminders for those without a regular dentist would have to be generated by another source, such as primary care providers or plans.
Respondents reported individual, provider and systemic factors as perceived barriers to dental care. Reported barriers are similar to previously reported barriers to dental care in Medicaid populations, and indicate the need for implementation of multiple strategies to affect improvement. A total of 62% of respondents reported at least one difficulty in seeing a dentist as often as needed, but reported difficulty was significantly less for children. In addition to respondents with a regular dentist, those with positive oral health were more likely to report no difficulties seeing a dentist. This population could be more connected to dental services and/or more attentive to oral care and report better oral health as a result. Individuals seeking care for urgent problems reported lower rates of timely access than those seeking routine care, and this could be a factor in those with fair or poor oral health reporting more difficulty seeing a dentist.
The most commonly reported difficulty in seeing a dentist was respondents´ fear of or nervousness about visiting a dentist (15%), which could possibly be improved through member level education. Prior studies have identified a lack of knowledge among Medicaid eligible families about accessing the system and using available resources7. In this study, 24% of respondents indicated that better communication about health plan benefits would facilitate care, and an equal number expressed dissatisfaction with the plan´s explanation of available dental benefits. Overall, 16% of respondents were not aware that their health plan has a dental benefit. The second most commonly reported barrier to care was contacting dentists who do not take Medicaid (14%). This could have been partly due to a lack of knowledge about participating providers. In comparing the two dental health vendors used by plans, respondents were statistically more likely to use the provider directory to locate a dentist if the vendor was Health Plex. Educational interventions about plan benefits, how to access them, and participating providers could assist in decreasing barriers to care experienced by respondents. Lack of coverage for needed services was cited often in open–ended responses; this issue should be further explored and may reflect a lack of education regarding benefits or unmet need.
The 2004 Access and Availability Survey found that 53% to 89% of dentists/sites made appointments within standard timeframes. A total of 74% of survey respondents with a regular dentist reported waiting less than one month for routine care, with an additional 21% within one to three months. New York City respondents and those who obtain care in private offices were more likely to obtain routine care appointments within one month.
_____________________________
* The Early and Periodic Screening, Diagnostic, and Treatment (EPSDT) program requires states to provide Medicaid enrollees under the age of 21 with periodic components of care, e.g., comprehensive health and developmental history, comprehensive physical examination, immunizations, and vision, hearing, and dental screening.
This may be related to numbers of participating providers, as well as patient volumes in hospital or community clinics with resultant longer wait times. Respondents reported more difficulty with acute problems, with only 35% of those seeking acute care waiting less than one day, and 27% waiting one to two days. The acuity of the problems for which care was sought was not defined in the study, and respondents´ problems may not be comparable to problems described in the Access and Availability survey. Discrepancies in perception of the acuity of problems between respondents and providers/sites could also impact appointment times. Despite the possible effect of these factors, there is considerable discrepancy between wait times for appointments for acute problems in this study and the Access and Availability survey. Since respondents to this question are those with a regular dentist, and therefore less likely to experience difficulty seeing a dentist, wait times for both acute and routine care could be worse for those without a regular dentist. Satisfaction with waiting times for appointments was the item for which respondents reported the highest rate of dissatisfaction (18%). Respondents in managed care reported better rates of timely appointments for routine care than respondents in FFS. However, since rates for timely access, both for routine and acute care, varied moderately among plans, plans should evaluate their individual rates and assess possible plan specific barriers to timely care.
Low numbers of participating providers treating Medicaid eligible individuals is an often– cited problem with access to care for this population. Geographic maldistribution of dentists contributes to inadequate access and unmet need1. A study of Medicaid eligible children´s access to dental care found children were more likely to receive care in counties with higher densities of dentists per enrollee8, and difficulty identifying participating providers has been reported as a significant barrier to care. "More dentists to choose from" was the most commonly cited facilitator to care among respondents. Difficulty scheduling and long wait times in waiting rooms, two commonly cited barriers, could be related to numbers of participating providers or particular providers. Low reimbursement rates and administrative complexities have been cited as factors negatively impacting dental clinician participation in Medicaid. Streamlining administrative processes, such as pre–approvals for anticipated services, could be beneficial in increasing provider participation and access2. More convenient hours as a facilitator and transportation as a barrier are common themes in the literature and in responses to the survey. Only 47% of respondents reported satisfaction with numbers of dentists to choose from. There is moderate variation of satisfaction responses among plans, including numbers of providers to choose from, and for wait times for appointments, which also varied among plans in the Access and Availability survey. Availability of providers could be further explored at the plan level.
Satisfaction
Previous studies have found that once access to dental care has been attained, most are satisfied9. Reported rates of satisfaction with overall care among respondents with a regular dentist were generally high, with 74% either somewhat or very satisfied, and 74% somewhat or very satisfied with dental advice received, higher for children.
Respondents were satisfied with staff friendliness//helpfulness (81%), in contrast to other studies that found staff attitudes to be problematic9. Respondents´ satisfaction with health plans was lower, with 24% reporting dissatisfaction with health plans´ explanation of benefits, particularly for adults, and 31% dissatisfaction with numbers of dentists to choose from. Educational initiatives about plan benefits offers significant opportunity for improvement; provider pool and availability should be further assessed.
MCO Differences
Overall, enrollees in MMC fared better for annual visits than FFS respondents, but there was variability among plans in several areas that present opportunities for improvement. In addition to wait times for routine care appointments and use of provider directories, moderate variation was found for timeframes for acute appointments and several satisfaction items such as numbers of dentists to choose from, and staff friendliness/helpfulness. Plans should further assess satisfaction and wait times for dental care for their members, and member access to provider information. Density of participating dental providers per enrollee affects access and could be reflected in waiting periods for appointments and satisfaction with the provider pool. The range of rates of visits to a dentist within the past year is similar to the range of rates for seeing a dentist on a regular basis. Efforts to encourage identification of a regular dentist, which is associated with increased annual dental visits and fewer difficulties seeing a dentist, could positively impact visit rates. Such efforts could include dissemination of plan provider and benefit information, and educational interventions regarding the need for regular dental visits.
Disparities
The national prevalence of untreated caries varies sociodemographically, with higher reported levels for black and Hispanic children than white children. Disparities in dental care utilization have been identified for elderly black populations and poor black children2, and national surveys have shown that annual dental visits vary significantly by race3. Among survey respondents, black members were more likely to receive routine appointments within one month and to be satisfied with numbers of dentists to choose from but were less likely to respond to the survey in both MMC and FFS cohorts. The proportion of members by race/ethnicity varied widely by health plans. Higher rates of satisfaction and timeliness of appointments reported by black members could be related to particular plans´ characteristics. Compared to white respondents, other races were more likely to report forgetting appointments as a barrier, and difficulty finding a dentist who speaks their language. Races other than white were more likely to report that reminders to visit the dentist would facilitate care, as would education about good dental care and dentists that speak their language. Reaching culturally diverse populations can positively enhance utilization of dental services10 and should be part of improvement interventions. White respondents were more likely to report that more dentists to choose from would facilitate care; this may also be related to plan characteristics and/or geographic maldistribution.
Study Limitations
Most limitations to the study are inherent in survey research. The response rate of 22.3% was relatively low, particularly with the implementation of two features to enhance response rates: a short survey and inclusion of English and Spanish surveys in each mail package. A potential impact to the generalizability of the results is that respondents differed from non–respondents on age, race/ethnicity, gender, NY region, and Medicaid aid type. The impact of these differences is most likely minimal, since there were large sample sizes, small demographic differences among the MMC cohort, and no differences noted in the comparison between the mail and telephone respondents. In addition, 29 separate logistic regressions were performed to determine the relationship of each of the five demographic variables with each of 29 dichotomized survey items. Very few variables yielded significance, further indicating that the response bias resulted in very little, if any bias.
Response bias is a potential limitation of the study, in that members who responded were probably more likely to have visited a dentist than non–respondents. Most respondents (82%) visited a dentist within the past two years, but the last dental visit for non–respondents is not known. Members who do not visit a dentist were probably less likely to complete the survey, resulting in higher rates of members reporting care, positively biasing the rates. It is possible that a corresponding advantage is respondents´ greater experience with care, which may increase their ability to rate care.
Recommendations
Survey findings of barriers to oral health are consistent with barriers identified in published reports, including knowledge of plan benefits, timely access to professional care and oral health behaviors. Although survey respondents´ reported access is better than that reported in HEDIS data, 62% of respondents reported difficulty in seeing a dentist as often as needed.
Respondents report a need for improved explanation of plan benefits, consistent with reports in the literature of Medicaid recipients´ difficulty accessing dental benefits. Educating Medicaid families on accessing the dental care system is necessary, as a lack of knowledge about available resources has impeded access to care7. Plans´ explanation of benefits elicited a relatively high rate of dissatisfaction among respondents. Plans could develop interventions to ensure that members are aware of dental benefits, how to access benefits and participating providers, and what is covered, and ensure that culturally diverse populations are reached.
Guidance on oral care behaviors as recommended for children could potentially benefit the adult population as well, and education could affect fear of visiting the dentist, the highest reported barrier to care. Educational interventions regarding oral care have been shown to have impact on behavior only if sustained11. Such educational intervention could be considered for inclusion in primary care visits. Increasing the number of members with regular dentists could improve access to ongoing guidance. Education of members about benefits and available providers could increase numbers of members with regular dentists and could possibly be facilitated by primary care providers through referrals.
Respondents were concerned about numbers of participating dentists to choose from; low numbers of participating providers is an often–reported barrier to access in the literature, with reimbursement and cumbersome administrative procedures cited as reasons for lack of participation. Some members indicated that dentists who speak their language would facilitate care. Analysis of plan specific participating provider pools, as well as geographic distribution of providers, could be an area for future study. Streamlining administrative procedures such as care approval processes has been cited as an intervention to enhance provider participation as well as care; plans should evaluate existing administrative procedures if believed to be a factor in accessing care.
Reminders to visit the dentist were cited as a possible facilitator by respondents; since many respondents did not have a regular dentist, plans or primary care providers could potentially generate such reminders to facilitate dental visits.
Further analysis of lack of coverage for needed services could be conducted to determine if it reflects true unmet need or lack of knowledge about covered services. In addition, an effectiveness of care process measure such as appropriate preventive use of fluoride treatment or dental sealants could be an area for future study.
|top of section| |top of page|REFERENCES
1. Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General. National Institute of Dental and Craniofacial Research, National Institute of Health.
Available here. Accessed December 28, 2006. 1
2. Stanton MW, Rutherford MK. Dental Care: improving access and quality. Rockville (MD): Agency for Healthcare Research and Quality; 2003. Research in Action Issue #13. AHRQ Pub No. 03–0040. 2
3. Center for Disease Control and Prevention, National Center for Health Statistics, Healthy People 2000 Final Review. Hyattsville, Maryland: Public Health Service 2001. Available at http://www.cdc.gov/nchs/data/hp2000/hp2k01. Accessed December 10, 2006. 3
4. Hughes D, Duderstadt K, Soobader M, Newacheck, P. (2005) Disparities in Children´s Use of Oral Health Services. Public Health Reports, 120: 455–462. 4
5. American Academy of Pediatrics Section on Pediatric Dentistry Policy Statement. Oral Health Risk Assessment Timing and Establishment of the Dental Home. (2003) Pediatrics, 111(5): 1113–1116. 5
6. Lewis CW, Grossman DC, Domoto PK, Deyo RA. (2000) The Role of the Pediatrician in the Oral Health of Children: A National Survey. Pediatrics, 106(6): e84. 6
7. Watson M, Manski R, Macek D. The impact of income on children´s and adolescents´ preventive dental visits. J Am Dental Assoc 2001; 132:1580–7. 7
8. VanLandeghem K, Bronstein J, Brach C. Children´s dental care access in Medicaid: the role of medical care use and dentist participation, CHIRI Issue Brief No.2. Rockville (MD): Agency for Healthcare Research and Quality; 2003 8
9. Mofidi M, Rozier RG, King RS. (2002) Problems with access to dental care for Medicaid– insured children: what caregivers think. Am J Public Health; 92(1): 53–58. 9
10. Mouradian, W. Wehr, E. Crall, J. (2000) Disparities in Children´s Oral Health and Access to Dental Care. JAMA 284(20):2625–2631. 10
11. Prevention of dental caries in preschool children: recommendations and rationale. US Preventive Services Task Force. Am J Prev Med 2004; 26(4): 326–329. 11
12. Beltran–Aguilar E, Barker LK, Canto MT. Surveillance for Dental Caries, Dental Sealants, Tooth Retention, Edentulism, and Enamel Fluorosis – United States 1988–1994 and 1999–2002. MMWR 2005; 54(03) 1–44. 12
ATTACHMENT 1
ADULT SURVEY
Si prefiere completar la encuesta en español use la encuesta adjunta, escrita en español.
If you prefer completing the survey in Spanish, use the enclosed Spanish survey instead.
To help us improve your dental care, we are requesting your opinions. Following is a short survey from the New York State Department of Health asking about your experience with dental care.
Please complete this short questionnaire and return it in the enclosed envelope. The survey asks questions regarding dental care you have received from your dentist, experience scheduling appointments, and problems you may have in seeing the dentist. Your answers will help us make dental care better for people with Medicaid health insurance.
Be assured that your answers to all the questions are completely private, confidential, and will not be shared with anyone. IPRO (an independent not–for–profit organization) will collect the surveys and prepare reports that summarize the answers from all of the surveys. The survey has an identification number for mailing purposes only. This is so we may check your name off the list when the survey is returned. Your name will never be placed on the survey, and at no point during this process will you be matched with your answers.
Please fill out the survey and send it back in the postage–paid envelope provided. Your help in collecting this information is voluntary. Please call IPRO toll–free at 1–800–852–3685, ext. 330 if you have any questions about the survey.
Your responses are very important and greatly appreciated.
Thank you for helping us make the New York State Medicaid dental program better for everyone.
Sincerely,
Foster Gesten, M.D.
Medical Director
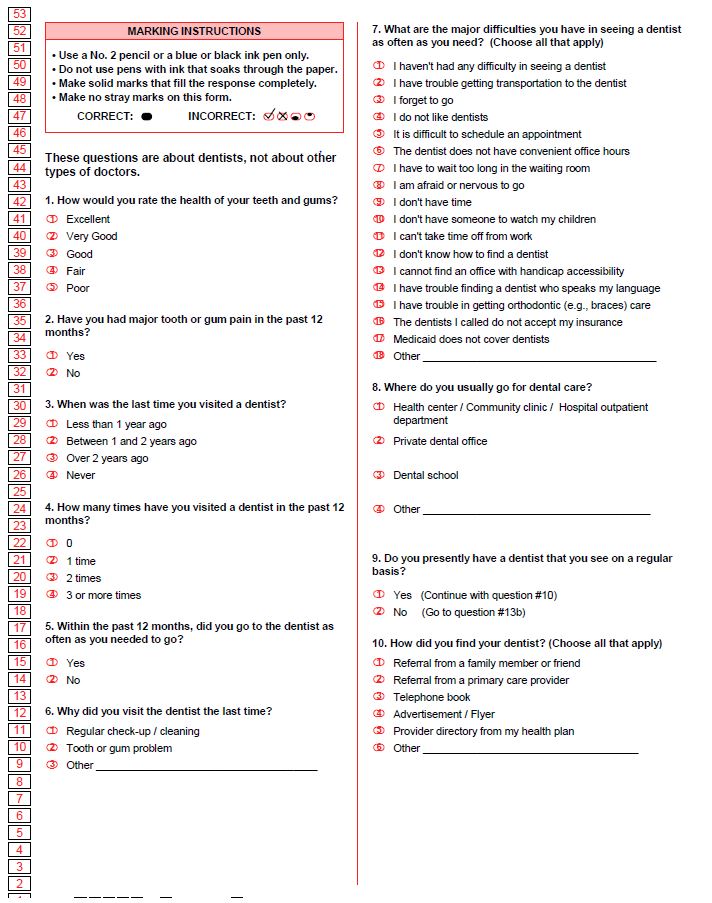
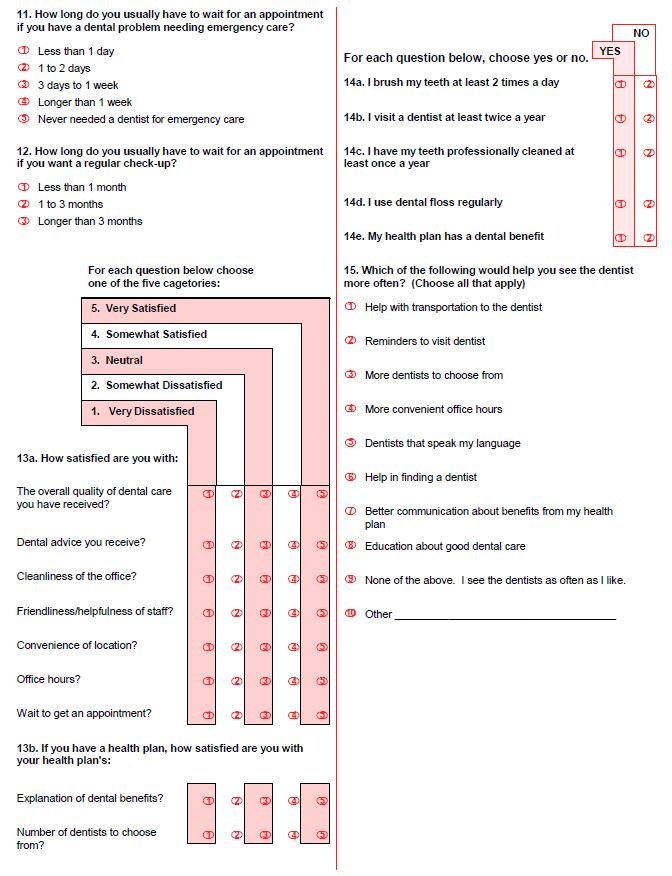
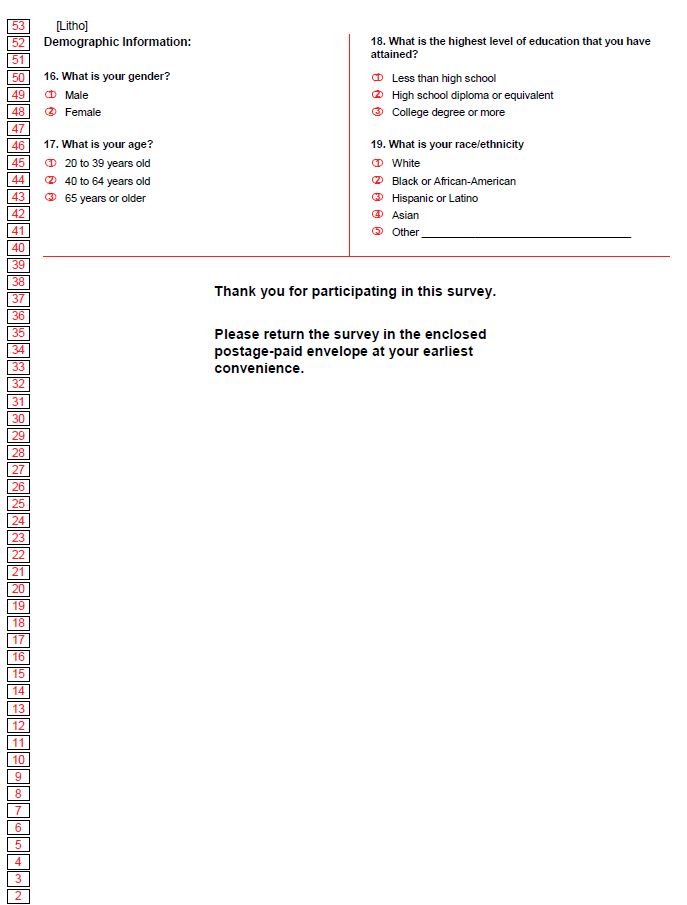
ATTACHMENT 2
CHILD SURVEY
Si prefiere completar la encuesta en español use la encuesta adjunta, escrita en español.
If you prefer completing the survey in Spanish, use the enclosed Spanish survey instead.
To help us improve your child´s dental care, we are requesting your opinions. Following is a short survey from the New York State Department of Health asking about your child´s experience with dental care. If you have more than one child, please answer the questions for the child named in the address above.
Please complete this short questionnaire, and return it in the enclosed envelope. The survey asks questions regarding dental care your child has received from your dentist, experience scheduling appointments, and problems your child may have in seeing the dentist. Your answers will help us make dental care better for people with Medicaid health insurance.
Be assured that your answers to all the questions are completely private, confidential, and will not be shared with anyone. IPRO (an independent not–for–profit organization) will collect the surveys and prepare reports that summarize the answers from all of the surveys. The survey has an identification number for mailing purposes only. This is so we may check your child´s name off the list when the survey is returned. Your name will never be placed on the survey, and at no point during this process will you be matched with your answers.
Please fill out the survey and send it back in the postage–paid envelope provided. Your help in collecting this information is voluntary. Please call IPRO toll–free at 1–800–852–3685, ext. 330 if you have any questions about the survey.
Your responses are very important and greatly appreciated.
Thank you for helping us make the New York State Medicaid dental program better for everyone.
Sincerely,
Foster Gesten, M.D.
Medical Director
ATTACHMENT 3
PHONE SURVEY QUESTIONS
How would you rate the health of your teeth and gums?
☐ Excellent
☐ Very Good
☐ Good
☐ Fair
☐ Poor
How many times have you visited a dentist in the past 12 months?
☐ 0
☐ 1 time
☐ 2 times
☐ 3 or more times
Do you presently have a dentist that you see on a regular basis?
☐ Yes (Continue with #4)
☐ No (Skip to #5)
How satisfied are you with the overall quality of dental care you have received?
☐ Very Satisfied
☐ Somewhat Satisfied
☐ Neutral
☐ Somewhat Dissatisfied
☐ Very Dissatisfied
Did you receive a survey from us about your Dental Care?
☐ Yes
☐ No
If yes: We´re trying to find: We´re trying to find the reasons why people may not have completed and sent back their surveys. May I ask if there was any particular reason why you didn´t complete the survey we sent you in the mail? (To the interviewer: Open–ended question. Don´t read choices).
☐ I am not a Medicaid patient
☐ It was too long
☐ I could not understand the questions
☐ The questions don´t apply to me
☐ I did not have time to fill it out
☐ I forgot to do it
☐ I lost it
☐ I did not go to the dentist
☐ Don´t know
☐ Other (please specify) ______________________________
Would you be more likely to complete a survey if it is by phone, by email, on the web, or some other way?
☐ Yes, by phone
☐ Yes, by email
☐ Yes, on the web
☐ Yes, some other way (Specify __________________________)
☐ No
ATTACHMENT 4
TABLES BY RESPONDENT CATEGORY
Background Characteristics of Respondents
| Survey Item | MMC | FFS | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Adult N = 952 |
Child N = 864 |
Adult N = 303 |
Child N = 211 |
|||||||
| n | % | n | % | n | % | n | % | |||
| 16 | Gender | |||||||||
| Male | 250 | 27.6 | 412 | 50.7 | 77 | 27.0 | 101 | 49.3 | ||
| Female | 656 | 72.4 | 401 | 49.3 | 208 | 73.0 | 104 | 50.7 | ||
| 17 | Age | |||||||||
| Adult | Child | |||||||||
| 20 – 39 | Less than 10 | 422 | 47.5 | 195 | 23.9 | 98 | 35.0 | 25 | 12.5 | |
| 40 – 64 | 10 – 19 | 454 | 51.1 | 621 | 76.1 | 179 | 63.9 | 175 | 87.5 | |
| 65 or over | 12 | 1.4 | 3 | 1.1 | ||||||
| 18 | Education | |||||||||
| Less than H.S. | 214 | 24.2 | 249 | 31.8 | 84 | 30.0 | 67 | 34.0 | ||
| High School | 461 | 52.1 | 383 | 48.9 | 159 | 56.8 | 95 | 48.2 | ||
| College degree or more | 209 | 23.6 | 151 | 19.3 | 37 | 13.2 | 35 | 17.8 | ||
| 19 | Race/ethnicity | |||||||||
| White | 302 | 34.6 | 247 | 32.1 | 157 | 57.1 | 78 | 40.6 | ||
| Black or African–American | 320 | 36.7 | 224 | 29.1 | 54 | 19.6 | 43 | 22.4 | ||
| Hispanic or Latino | 177 | 20.3 | 220 | 28.6 | 48 | 17.5 | 53 | 27.6 | ||
| Asian | 63 | 7.2 | 57 | 7.4 | 11 | 4.0 | 9 | 4.7 | ||
| Native American (open–ended response) | 6 | 0.7 | 4 | 0.5 | 3 | 1.1 | 3 | 1.6 | ||
| Arab (open–ended response) | 2 | 0.2 | 10 | 1.3 | 1 | 0.4 | 0 | 0.0 | ||
| Mixed Race (open–ended response) | 3 | 0.3 | 7 | 0.9 | 1 | 0.4 | 6 | 3.1 | ||
Oral Health Status
| Survey Item | MMC | FFS | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Adult | Child | Adult | Child | |||||||
| n | % | n | % | n | % | n | % | |||
| 1 | Health of teeth/gums | |||||||||
| Excellent | 54 | 5.8 | 145 | 17.0 | 13 | 4.4 | 32 | 15.2 | ||
| Very good | 150 | 16.0 | 219 | 25.6 | 38 | 12.8 | 49 | 23.3 | ||
| Good | 298 | 31.7 | 316 | 37.0 | 77 | 25.9 | 82 | 39.0 | ||
| Fair | 265 | 28.2 | 141 | 16.5 | 83 | 27.9 | 39 | 18.6 | ||
| Poor | 172 | 18.3 | 34 | 4.0 | 86 | 29.0 | 8 | 3.8 | ||
| 2 | Had major tooth or gum pain in the past 12 months | |||||||||
| Yes | 406 | 44.0 | 180 | 21.0 | 138 | 47.4 | 52 | 24.8 | ||
| No | 516 | 56.0 | 676 | 79.0 | 153 | 52.6 | 158 | 75.2 | ||
Dental Care Information
| Survey Item | MMC | FFS | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Adult | Child | Adult | Child | |||||||
| n | % | n | % | n | % | n | % | |||
| 3 | Last time visited a dentist | |||||||||
| Less than 1 year ago | 538 | 57.2 | 605 | 70.5 | 143 | 47.8 | 136 | 64.8 | ||
| Between 1 and 2 years ago | 189 | 20.1 | 151 | 17.6 | 55 | 18.4 | 36 | 17.1 | ||
| Over 2 years ago | 181 | 19.2 | 57 | 6.6 | 90 | 30.1 | 27 | 12.9 | ||
| Never | 33 | 3.5 | 45 | 5.2 | 11 | 3.7 | 11 | 5.2 | ||
| 4 | Number of times visited a dentist in the past 12 months | |||||||||
| 0 | 274 | 29.1 | 172 | 20.0 | 129 | 43.1 | 57 | 27.3 | ||
| 1 time | 238 | 25.3 | 263 | 30.7 | 48 | 16.1 | 52 | 24.9 | ||
| 2 times | 226 | 24.0 | 275 | 32.1 | 54 | 18.1 | 63 | 30.1 | ||
| 3 or more times | 204 | 21.7 | 148 | 17.2 | 68 | 22.7 | 37 | 17.7 | ||
| 5 | Whether went to the dentist as often as needed within the past 12 months | |||||||||
| Yes | 365 | 39.1 | 535 | 62.8 | 114 | 38.6 | 122 | 57.8 | ||
| No | 568 | 60.9 | 317 | 37.2 | 181 | 61.4 | 89 | 42.2 | ||
| 6 | Reason visited dentist last time | |||||||||
| Regular check–up / cleaning | 359 | 42.6 | 575 | 74.6 | 94 | 38.1 | 145 | 75.9 | ||
| Tooth or gum problem | 449 | 53.3 | 178 | 23.1 | 139 | 56.3 | 41 | 21.5 | ||
| Dentures (open–ended response) | 32 | 3.8 | 0 | 0 | 14 | 5.7 | 0 | 0 | ||
| Braces (open–ended response) | 2 | 0.2 | 18 | 2.3 | 0 | 0.0 | 5 | 2.6 | ||
| 8 | Where usually go for dental care | |||||||||
| Health center / Community clinic / Hospital outpatient department | 213 | 24.5 | 229 | 28.8 | 112 | 42.1 | 91 | 46.4 | ||
| Private dental office | 632 | 72.8 | 548 | 68.8 | 141 | 53.0 | 96 | 49.0 | ||
| Dental school | 7 | 0.8 | 11 | 1.4 | 5 | 1.9 | 7 | 3.6 | ||
| Don´t go (open–ended response) | 16 | 1.8 | 8 | 1.0 | 8 | 3.0 | 2 | 1.0 | ||
| 9 | Have a dentist to see on a regular basis | |||||||||
| Yes | 534 | 59.0 | 627 | 76.0 | 151 | 52.1 | 150 | 73.9 | ||
| No | 371 | 41.0 | 198 | 24.0 | 139 | 47.9 | 53 | 26.1 | ||
| 14a | Brush teeth at least 2 times a day | |||||||||
| Yes | 747 | 83.3 | 667 | 79.2 | 193 | 68.4 | 176 | 84.2 | ||
| No | 150 | 16.7 | 175 | 20.8 | 89 | 31.6 | 33 | 15.8 | ||
| 14b | Visit a dentist at least twice a year | |||||||||
| Yes | 420 | 47.5 | 535 | 63.6 | 111 | 39.9 | 128 | 62.4 | ||
| No | 464 | 52.5 | 306 | 36.4 | 167 | 60.1 | 77 | 37.6 | ||
| 14c | Have teeth professionally cleaned at least once a year | |||||||||
| Yes | 472 | 51.6 | 589 | 70.3 | 118 | 41.4 | 143 | 69.1 | ||
| No | 442 | 48.4 | 249 | 29.7 | 167 | 58.6 | 64 | 30.9 | ||
| 14d | Use dental floss regularly | |||||||||
| Yes | 402 | 45.6 | 283 | 33.9 | 113 | 41.2 | 85 | 41.5 | ||
| No | 480 | 54.4 | 551 | 66.1 | 161 | 58.8 | 120 | 58.5 | ||
Barriers/Facilitators to Care
| Survey Item | MMC | FFS | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Adult | Child | Adult | Child | ||||||
| n | % | n | % | n | % | n | % | ||
| 7@ | Major difficulties had in seeing a dentist as often as needed | ||||||||
| Have not had difficulty in seeing a dentist | 274 | 30.8 | 372 | 47.0 | 75 | 26.1 | 95 | 49.5 | |
| Have trouble getting transportation | 85 | 9.6 | 66 | 8.3 | 43 | 15.0 | 24 | 12.5 | |
| Forget to go | 79 | 8.9 | 54 | 6.8 | 26 | 9.1 | 10 | 5.2 | |
| Do not like my dentist / dentists in general | 165 | 18.6 | 53 | 6.7 | 58 | 20.2 | 10 | 5.2 | |
| It is difficult to schedule an appt. | 101 | 11.4 | 95 | 12.0 | 28 | 9.8 | 24 | 12.5 | |
| Dentist does not have convenient office hours | 44 | 4.9 | 55 | 7.0 | 15 | 5.2 | 8 | 4.2 | |
| Have to wait too long in the waiting room | 100 | 11.2 | 83 | 10.5 | 32 | 11.1 | 17 | 8.9 | |
| Afraid or nervous to go | 166 | 18.7 | 89 | 11.3 | 54 | 18.8 | 20 | 10.4 | |
| Don´t have time | 58 | 6.5 | 16 | 2.0 | 11 | 3.8 | 7 | 3.6 | |
| Don´t have someone to watch children | 43 | 4.8 | 9 | 1.1 | 12 | 4.2 | 1 | 0.5 | |
| Can´t take time off from work | 42 | 4.7 | 34 | 4.3 | 10 | 3.5 | 7 | 3.6 | |
| Don´t know how to find a dentist | 58 | 6.5 | 25 | 3.2 | 21 | 7.3 | 8 | 4.2 | |
| Cannot find office with handicap accessibility | 5 | 0.6 | 4 | 0.5 | 3 | 1.0 | 0 | 0.0 | |
| Have trouble finding a dentist who speaks my language | 48 | 5.4 | 36 | 4.6 | 9 | 3.1 | 4 | 2.1 | |
| Have trouble getting orthodontic care | 47 | 5.3 | 67 | 8.5 | 18 | 6.3 | 11 | 5.7 | |
| The dentists I called do not accept my insurance | 157 | 17.7 | 77 | 9.7 | 63 | 22.0 | 25 | 13.0 | |
| Medicaid does not cover dentists | 60 | 6.7 | 28 | 3.5 | 31 | 10.8 | 9 | 4.7 | |
| 7@ | Major difficulties in seeing a dentist as often as needed | ||||||||
| Other (open–ended responses): | 62 | 7.0 | 33 | 4.2 | 26 | 9.1 | 9 | 4.7 | |
| Have no teeth | 1 | 0 | 2 | 0 | |||||
| Medicaid does not cover services I need | 25 | 7 | 4 | 0 | |||||
| Office location not convenient | 3 | 8 | 3 | 1 | |||||
| Do not have Medicaid / insurance / card | 11 | 2 | 3 | 2 | |||||
| Unclean office | 3 | 2 | 0 | 0 | |||||
| Other medical problems | 1 | 1 | 3 | 3 | |||||
| Expense / out–of–pocket costs | 6 | 1 | 0 | 0 | |||||
| Medicaid dentists are not good | 7 | 4 | 3 | 0 | |||||
| Not enough choices of dentists in Medicaid | 2 | 3 | 5 | 3 | |||||
| Other | 3 | 5 | 3 | 0 | |||||
| 14e | My health plan has a dental benefit | ||||||||
| Yes | 690 | 79.7 | 701 | 87.8 | 188 | 74.0 | 156 | 83.4 | |
| No | 176 | 20.3 | 97 | 12.2 | 66 | 26.0 | 31 | 16.6 | |
| 15@ | What would help see the dentist more often | ||||||||
| None. I see the dentists as often as I like. | 150 | 17.1 | 213 | 26.9 | 48 | 18.0 | 46 | 23.2 | |
| Help with transportation to the dentist | 130 | 14.8 | 123 | 15.5 | 54 | 20.2 | 40 | 20.2 | |
| Reminders to visit dentist | 267 | 30.5 | 246 | 31.0 | 71 | 26.6 | 65 | 32.8 | |
| More dentists to choose from | 303 | 34.6 | 224 | 28.2 | 108 | 40.4 | 61 | 30.8 | |
| More convenient office hours | 138 | 15.8 | 160 | 20.2 | 45 | 16.9 | 34 | 17.2 | |
| Dentists that speak my language | 146 | 16.7 | 102 | 12.9 | 40 | 15.0 | 27 | 13.6 | |
| Help in finding a dentist | 160 | 18.3 | 88 | 11.1 | 65 | 24.3 | 29 | 14.6 | |
| Better communication about benefits from my health plan | 252 | 28.8 | 153 | 19.3 | 64 | 24.0 | 41 | 20.7 | |
| Education about good dental care | 139 | 15.9 | 117 | 14.8 | 32 | 12.0 | 28 | 14.1 | |
| 15@ | What would help see the dentist more often | ||||||||
| Other (open–ended responses): | 66 | 7.5 | 46 | 5.8 | 29 | 10.9 | 5 | 2.5 | |
| Faster appointment times | 4 | 4 | 4 | 1 | |||||
| Closer location | 6 | 9 | 5 | 1 | |||||
| Handicap accessible | 0 | 1 | 0 | 0 | |||||
| Help with anxiety | 7 | 4 | 2 | 1 | |||||
| Equal treatment for Medicaid patients | 4 | 0 | 0 | 1 | |||||
| Less waiting time at dental Office | 0 | 2 | 1 | 1 | |||||
| Want more specific dental benefits covered | 28 | 16 | 9 | 0 | |||||
| Better price | 5 | 0 | 0 | 0 | |||||
| I have no teeth / have dentures | 2 | 0 | 3 | 0 | |||||
| Better dentists to choose From | 6 | 8 | 4 | 0 | |||||
| Faster approval from Medicaid | 3 | 1 | 1 | 0 | |||||
| Other | 1 | 1 | 0 | 0 | |||||
@ Multiple responses
Access and Availability of Dental Care
| Survey Item | MMC | FFS | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Adult | Child | Adult | Child | ||||||
| n | % | n | % | n | % | n | % | ||
| 10@ ◆ |
How found dentist | ||||||||
| Referral from family / friend | 191 | 36.8 | 189 | 31.8 | 72 | 52.2 | 64 | 44.8 | |
| Referral from a PCP / doctor / nurse | 87 | 16.8 | 115 | 19.3 | 22 | 15.9 | 33 | 23.1 | |
| Telephone book | 26 | 5.0 | 21 | 3.5 | 22 | 15.9 | 19 | 13.3 | |
| Advertisement / Flyer | 16 | 3.1 | 23 | 3.9 | 10 | 7.2 | 5 | 3.5 | |
| Provider directory from plan | 216 | 41.6 | 286 | 48.1 | 28 | 20.3 | 29 | 20.3 | |
| Other (open–ended responses): In local neighborhood, walk–in Using long–term dentist Other |
21 14 5 2 |
4.0 | 14 10 3 1 |
2.4 | 3 2 1 |
2.2 | 5 4 1 |
3.5 | |
| 11 ◆ | How long usually have to wait for an appt. if have a dental problem | ||||||||
| Less than 1 day | 130 | 24.8 | 151 | 24.5 | 36 | 24.2 | 30 | 20.4 | |
| 1 to 2 days | 120 | 22.9 | 102 | 16.6 | 33 | 22.1 | 36 | 24.5 | |
| 3 days to 1 week | 92 | 17.6 | 103 | 16.7 | 25 | 16.8 | 14 | 9.5 | |
| Longer than 1 week | 55 | 10.5 | 60 | 9.7 | 19 | 12.8 | 10 | 6.8 | |
| Never needed a dentist for emergency care | 127 | 24.2 | 200 | 32.5 | 36 | 24.2 | 57 | 38.8 | |
| 12 ◆ | How long usually have to wait for an appt. if want a regular check–up | ||||||||
| Less than 1 month | 385 | 73.9 | 450 | 73.9 | 82 | 55.8 | 98 | 66.7 | |
| 1 to 3 months | 105 | 20.2 | 130 | 21.3 | 53 | 36.1 | 39 | 26.5 | |
| Longer than 3 months | 31 | 6.0 | 29 | 4.8 | 12 | 8.2 | 10 | 6.8 | |
@ Multiple responses
◆ Items based on skip pattern; rates based on respondents with a regular dentist.
Satisfaction with Dental Care
| Survey Item | MMC | FFS | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Adult | Child | Adult | Child | ||||||
| n | % | n | % | n | % | n | % | ||
| 13a ◆ |
Satisfaction with overall quality of dental care received | ||||||||
| Very satisfied | 219 | 45.4 | 322 | 53.2 | 68 | 48.6 | 83 | 57.2 | |
| Somewhat satisfied | 124 | 25.7 | 142 | 23.5 | 33 | 23.6 | 31 | 21.4 | |
| Neutral | 77 | 16.0 | 81 | 13.4 | 22 | 15.7 | 15 | 10.3 | |
| Somewhat dissatisfied | 32 | 6.6 | 28 | 4.6 | 9 | 6.4 | 7 | 4.8 | |
| Very dissatisfied | 30 | 6.2 | 32 | 5.3 | 8 | 5.7 | 9 | 6.2 | |
| 13a ◆ |
Satisfaction with dental advice received | ||||||||
| Very satisfied | 210 | 44.6 | 312 | 52.6 | 68 | 48.9 | 85 | 59.9 | |
| Somewhat satisfied | 116 | 24.6 | 152 | 25.6 | 29 | 20.9 | 26 | 18.3 | |
| Neutral | 83 | 17.6 | 68 | 11.5 | 22 | 15.8 | 15 | 10.6 | |
| Somewhat dissatisfied | 34 | 7.2 | 32 | 5.4 | 16 | 11.5 | 12 | 8.5 | |
| Very dissatisfied | 28 | 5.9 | 29 | 4.9 | 4 | 2.9 | 4 | 2.8 | |
| 13a ◆ |
Satisfaction with cleanliness of the office | ||||||||
| Very satisfied | 301 | 61.4 | 376 | 63.4 | 93 | 64.6 | 100 | 70.9 | |
| Somewhat satisfied | 98 | 20.0 | 111 | 18.7 | 26 | 18.1 | 26 | 18.4 | |
| Neutral | 49 | 10.0 | 54 | 9.1 | 15 | 10.4 | 9 | 6.4 | |
| Somewhat dissatisfied | 19 | 3.9 | 25 | 4.2 | 6 | 4.2 | 2 | 1.4 | |
| Very dissatisfied | 23 | 4.7 | 27 | 4.6 | 4 | 2.8 | 4 | 2.8 | |
| 13a ◆ |
Satisfaction with friendliness/helpfulness of staff | ||||||||
| Very satisfied | 301 | 60.6 | 354 | 58.8 | 95 | 66.4 | 94 | 67.1 | |
| Somewhat satisfied | 100 | 20.1 | 130 | 21.6 | 28 | 19.6 | 30 | 21.4 | |
| Neutral | 51 | 10.3 | 58 | 9.6 | 10 | 7.0 | 9 | 6.4 | |
| Somewhat dissatisfied | 19 | 3.8 | 30 | 5.0 | 6 | 4.2 | 4 | 2.9 | |
| Very dissatisfied | 26 | 5.2 | 30 | 5.0 | 4 | 2.8 | 3 | 2.1 | |
| 13a ◆ |
Satisfaction with convenience of location | ||||||||
| Very satisfied | 299 | 63.6 | 344 | 57.4 | 81 | 60.0 | 85 | 61.2 | |
| Somewhat satisfied | 91 | 19.4 | 124 | 20.7 | 23 | 17.0 | 30 | 21.6 | |
| Neutral | 37 | 7.9 | 59 | 9.8 | 19 | 14.1 | 13 | 9.4 | |
| Somewhat dissatisfied | 16 | 3.4 | 32 | 5.3 | 6 | 4.4 | 5 | 3.6 | |
| Very dissatisfied | 27 | 5.7 | 40 | 6.7 | 6 | 4.4 | 6 | 4.3 | |
| 13a ◆ |
Satisfaction with office hours | ||||||||
| Very satisfied | 234 | 49.9 | 296 | 50.6 | 78 | 58.6 | 73 | 52.1 | |
| Somewhat satisfied | 126 | 26.9 | 158 | 27.0 | 29 | 21.8 | 42 | 30.0 | |
| Neutral | 46 | 9.8 | 66 | 11.3 | 18 | 13.5 | 15 | 10.7 | |
| Somewhat dissatisfied | 41 | 8.7 | 24 | 4.1 | 4 | 3.0 | 4 | 2.9 | |
| Very dissatisfied | 22 | 4.7 | 41 | 7.0 | 4 | 3.0 | 6 | 4.3 | |
| 13a ◆ |
Satisfaction with wait to get an appointment | ||||||||
| Very satisfied | 198 | 42.2 | 257 | 43.8 | 60 | 44.1 | 62 | 44.3 | |
| Somewhat satisfied | 137 | 29.2 | 131 | 22.3 | 28 | 20.6 | 38 | 27.1 | |
| Neutral | 50 | 10.7 | 89 | 15.2 | 23 | 16.9 | 12 | 8.6 | |
| Somewhat dissatisfied | 48 | 10.2 | 54 | 9.2 | 17 | 12.5 | 19 | 13.6 | |
| Very dissatisfied | 36 | 7.7 | 56 | 9.5 | 8 | 5.9 | 9 | 6.4 | |
◆ Items based on skip pattern; rates based on respondents with a regular dentist.
Satisfaction with Health Plan
| Survey Item | MMC | FFS | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Adult | Child | Adult | Child | ||||||
| n | % | n | % | n | % | n | % | ||
| 13b | Satisfaction with health plan´s explanation of dental benefits | ||||||||
| Very satisfied | 218 | 27.4 | 302 | 38.9 | 74 | 29.7 | 68 | 35.8 | |
| Somewhat satisfied | 168 | 21.1 | 187 | 24.1 | 45 | 18.1 | 44 | 23.2 | |
| Neutral | 175 | 22.0 | 150 | 19.3 | 53 | 21.3 | 34 | 17.9 | |
| Somewhat dissatisfied | 95 | 11.9 | 67 | 8.6 | 37 | 14.9 | 16 | 8.4 | |
| Very dissatisfied | 141 | 17.7 | 70 | 9.0 | 40 | 16.1 | 28 | 14.7 | |
| 13b | Satisfaction with number of dentists to choose from | ||||||||
| Very satisfied | 185 | 24.1 | 224 | 30.3 | 51 | 21.5 | 48 | 26.8 | |
| Somewhat satisfied | 147 | 19.1 | 149 | 20.2 | 34 | 14.3 | 35 | 19.6 | |
| Neutral | 164 | 21.4 | 165 | 22.3 | 44 | 18.6 | 35 | 19.6 | |
| Somewhat dissatisfied | 108 | 14.1 | 71 | 9.6 | 43 | 18.1 | 25 | 14.0 | |
| Very dissatisfied | 164 | 21.4 | 130 | 17.6 | 65 | 27.4 | 36 | 20.1 | |
ATTACHMENT 5
VENDOR TABLES
Table A–1. Comparison of Plans based on Vendor Utilization
| Survey Item | Plans without Dental Vendor (n=519) |
Plans with Dental Vendor (n=1,297) |
p value | |
|---|---|---|---|---|
| Background Characteristics of Respondents | ||||
| 16 | Male gender | 43.0% | 36.8% | n.s. |
| 18 | High school graduate | 66.9% | 74.3% | n.s. |
| 19 | Race/ethnicity | 0.0001 | ||
| White | 27.3% | 35.9% | ||
| Black or African–American | 30.1% | 34.4% | ||
| Hispanic or Latino | 33.9% | 20.3% | ||
| Other | 8.7% | 9.5% | ||
| Oral Health Status | ||||
| 1 | Health of teeth/gums is excellent, very good, or good | 69.1% | 64.6% | n.s. |
| 2 | Had major tooth or gum pain in the past 12 months | 34.5% | 32.4% | n.s. |
| Dental Care Information | ||||
| 3 | Visited a dentist < 1 year ago | 60.1% | 64.9% | n.s. |
| 4 | Visited a dentist 1+ times in the past 12 months | 75.3% | 75.2% | n.s. |
| 5 | Went to the dentist as often as needed within the past 12 months | 49.1% | 50.9% | n.s. |
| 6 | Visited dentist last time for regular check–up / cleaning | 58.6% | 57.6% | n.s. |
| 8 | Usually get dental care at private office | 63.6% | 75.2% | 0.0001 |
| 9 | Have a dentist to see on a regular basis | 64.1% | 68.3% | n.s. |
| 14a | Brush teeth at least 2 times a day | 79.9% | 81.9% | n.s. |
| 14b | Visit a dentist at least 2 times a year | 52.6% | 56.5% | n.s. |
| 14c | Have teeth professionally cleaned 1+ a year | 56.9% | 62.0% | n.s. |
| 14d | Use dental floss regularly | 36.8% | 41.1% | n.s. |
| Barriers/Facilitators to Care | ||||
| 7 | No major difficulties in seeing a dentist as often as needed | 38.8% | 38.3% | n.s. |
| 14e | My health plan has a dental benefit | 85.8% | 82.7% | n.s. |
| 15 | Nothing would help me see the dentist more often | 21.2% | 22.0% | n.s. |
| Access and Availability of Dental Care | ||||
| 10 @ ◆ |
How found dentist | |||
| Referral from family / friend | 42.5% | 31.0% | 0.0001 | |
| Referral from a PCP / doctor / nurse | 18.6% | 18.0% | n.s. | |
| Provider directory from plan | 34.6% | 49.0% | 0.0001 | |
| Other | 10.6% | 10.3% | n.s. | |
| 11 ◆ | Usually wait < 1 day for an appt. for dental problem | 33.0% | 35.1% | n.s. |
| 12 ◆ | Usually wait < 1 month for an appt. for regular check–up | 79.7% | 71.8% | n.s. |
| Very / Somewhat Satisfied with: | ||||
| 13a ◆ |
Overall quality of dental care received | 74.5% | 74.2% | n.s. |
| Dental advice received | 74.4% | 74.2% | n.s. | |
| Cleanliness of the office | 83.3% | 81.3% | n.s. | |
| Friendliness/helpfulness of staff | 81.8% | 80.0% | n.s. | |
| Convenience of location | 83.5% | 79.1% | n.s. | |
| Office hours | 77.8% | 77.0% | n.s. | |
| Wait to get an appointment | 73.6% | 66.6% | n.s. | |
| 13b | Health plan´s explanation of dental benefits | 55.4% | 55.7% | n.s. |
| Number of dentists to choose from | 48.9% | 46.0% | n.s. | |
Note: Bold values represent the statistically higher value in that row.
@ Multiple responses
◆ Items based on skip pattern; rates based on respondents with a regular dentist.
Table A–2. Comparison of Plans Based on Specific Vendor
| Survey Item | Plans using HealthPlex (n=765) |
Plans using Doral (n=532) |
p value |
|
|---|---|---|---|---|
| Background Characteristics of Respondents | ||||
| 16 | Male gender | 36.0% | 37.8% | n.s. |
| 18 | High school graduate | 74.0% | 74.7% | n.s. |
| 19 | Race/ethnicity | n.s. | ||
| White | 34.2% | 38.3% | ||
| Black or African–American | 37.4% | 29.9% | ||
| Hispanic or Latino | 18.9% | 22.2% | ||
| Other | 9.4% | 9.6% | ||
| Oral Health Status | ||||
| 1 | Health of teeth/gums is excellent, very good, or good | 63.8% | 65.7% | n.s. |
| 2 | Had major tooth or gum pain in the past 12 months | 30.6% | 34.9% | n.s. |
| Dental Care Information | ||||
| 3 | Visited a dentist < 1 year ago | 64.5% | 65.6% | n.s. |
| 4 | Visited a dentist 1+ times in the past 12 months | 74.4% | 76.4% | n.s. |
| 5 | Went to the dentist as often as needed within the past 12 months | 48.3% | 54.7% | n.s. |
| 6 | Visited dentist last time for regular check–up / cleaning | 58.9% | 55.8% | n.s. |
| 8 | Usually get dental care at private office | 74.8% | 75.7% | n.s. |
| 9 | Have a dentist to see on a regular basis | 68.7% | 67.7% | n.s. |
| 14a | Brush teeth at least 2 times a day | 84.4% | 78.2% | n.s. |
| 14b | Visit a dentist at least 2 times a year | 55.7% | 57.5% | n.s. |
| 14c | Have teeth professionally cleaned 1+ a year | 61.3% | 63.0% | n.s. |
| 14d | Use dental floss regularly | 39.5% | 43.5% | n.s. |
| Barriers/Facilitators to Care | ||||
| 7 | No major difficulties in seeing a dentist as often as needed | 37.1% | 40.1% | n.s. |
| 14e | My health plan has a dental benefit | 83.4% | 81.6% | n.s. |
| 15 | Nothing would help me see the dentist more often | 20.8% | 23.7% | n.s. |
| Access and Availability of Dental Care | ||||
| 10 @ ◆ | How found dentist | |||
| Referral from family / friend | 23.0% | 42.6% | 0.0001 | |
| Referral from a PCP / doctor / nurse | 18.3% | 17.5% | n.s. | |
| Provider directory from plan | 55.6% | 39.3% | 0.0001 | |
| Other | 9.5% | 11.5% | n.s. | |
| 11 ◆ | Usually wait < 1 day for an appt. for dental problem | 32.6% | 38.3% | n.s. |
| 12 ◆ | Usually wait < 1 month for an appt. for regular check–up | 69.0% | 75.9% | n.s. |
| Very / Somewhat Satisfied with: | ||||
| 13a ◆ | Overall quality of dental care received | 74.5% | 73.6% | n.s. |
| Dental advice received | 73.7% | 74.9% | n.s. | |
| Cleanliness of the office | 80.5% | 82.3% | n.s. | |
| Friendliness/helpfulness of staff | 78.8% | 81.9% | n.s. | |
| Convenience of location | 78.3% | 80.2% | n.s. | |
| Office hours | 74.0% | 81.4% | n.s. | |
| Wait to get an appointment | 63.3% | 71.5% | n.s. | |
| 13b | Health plan´s explanation of dental benefits | 57.0% | 53.8% | n.s. |
| Number of dentists to choose from | 45.1% | 47.3% | n.s. | |
Note: Bold values represent the statistically higher value in that row.
@ Multiple responses
◆ Items based on skip pattern; rates based on respondents with a regular dentist.
