Pathways to Becoming Compliant with CMS Conflict of Interest Requirements
- Presentation is also available in Portable Document Format (PDF)
Nursing Home Transition and Diversion (NHTD) Waiver Program And Traumatic Brain Injury (TBI) Waiver Program
January 11, 2019
Topics for Discussion
- Introductions
- NHTD and TBI Waiver Updates
- HCBS Final Rule
- CMS Conflict of Interest Requirements
- For Discussion: Potential Conflict of Interest Compliant Models
NHTD and TBI Waiver Updates
- The TBI waiver renewal application has been approved by CMS through August 31, 2022.
- The NHTD waiver renewal application has been approved by CMS through June 30, 2023.
- Housing Payment Agent Contract
- Through a competitive process, the contract has been awarded to Public Partnerships LLC.
- Contract now includes both TBI and NHTD housing.
- DOH Team is currently updating NHTD and TBI program manuals and expects to distribute them to stakeholders for comment in February.
- DOH is in the process of preparing a crosswalk of previous qualifications vs. currently approved qualifications which will be presented for stakeholder comment. DOH will schedule a work group meeting to discuss crosswalk and comments in the near future.
- We will be seeking an amendment to grandfather in existing SC staff that do not meet new/current qualifications.
- To potentially help with capacity for service coordination, CIC and ILST, DOH will be seeking to amend both NHTD and TBI applications to address provider qualifications.
- CMS has also been advised that DOH will seek an amendment to address service limit caps imposed on the TBI waiver where there are currently no provisions for exceptions (i.e., circumstances where DOH may approve authorizations above the limits).
- The rate increases for TBI to address the Fair Labor Standards Act (FLSA) requirements, retroactive to October 13, 2015, is currently in review by CMS. The new rate will be implemented by the end of January. The rate increase for NHTD was implemented in July 2017.
- The minimum wage rate increase for TBI was submitted to CMS and is currently under review. Upon approval by CMS, NYSDOH will submit the same request to CMS for NHTD. This approach to submitting amendments for approval was requested by CMS.
- The minimum wage rate increases are submitted to the Division of Budget (DOB) and are pending approval.
- The minimum wage rate increase will include both 2018 and 2019 rate increments and will be included in the 2019 rate.
Home and Community Based Services (HCBS) Final Rule
- Enacted effective March 17, 2014 – relates to the provision of HCBS authorized under 1915(c) and 1915(i) waiver authorities (latter includes CFCO).
- Three Key Components of the HCBS Final Rule:
- Defines, describes and aligns home and community–based setting requirements;
- Defines person–centered planning requirements; and
- Defines conflict of interest provisions.
More information on the HCBS Final Regulation can be found here.
HCBS Final Rule: Settings Requirements
- Establishes that HCBS must be delivered in settings that meet defined criteria (e.g., is integrated and supports access to the greater community, facilitates choice regarding services and supports and who provides them).
- In general, institutional settings and settings that have the qualities of an institutional setting do not qualify as compliant "home and community–based settings".
- See Appendix for more information about definitions for compliant settings.
- NYSDOH received CMS approval of its Statewide Transition Plan (STP) November 16, 2018 to become fully compliant with the settings rule by March 1, 2022.
The State´s Transition Plan can be found here.
- What does this mean for NHTD and TBI Waivers?
- This may result in assessment of structured day program sites and home visits in the natural course of service provision.
- Additional activities will be needed by providers and the RRDCs to ensure compliance.
- DOH will be providing updates, information and additional guidance over the next couple of months.
HCBS Final Rule: Person–Centered Service Planning Requirements
- What does this mean for the NHTD and TBI waivers?
- NHTD and TBI are generally already compliant with person–centered service planning requirements.
- DOH team will include person–centered planning requirement changes in their respective program manuals.
CMS Conflict of Interest (COI) Requirements
- With much discussion, CMS agreed to extend the date for which the TBI and NHTD waivers must meet Conflict of Interest Requirements from January 1, 2019 to January 1, 2021.
- DOH will submit a technical amendment to the waiver to make this change, effective January 1, 2019 – DOH and CMS are prioritizing the wage amendments.
- Our goal is work collaboratively with you (providers and stakeholders) and CMS, to explore and implement approaches that are compliant with COI and to the maximum extent possible preserve continuity of care, choice, provider stability, and capacity and access to services.
- As discussed later, we will need to work collaboratively under short timeframes to ensure there is sufficient time to ensure a smooth transition to COI compliance and that reflects the goals of above.
HCBS Final Rule: Conflict of Interest (COI)
- Service Coordination activities must be independent of direct waiver service provision.
- Conflict occurs not just if the entity is a provider but if the entity:
- Has an interest in a provider, or
- Is employed by a provider.
- Requirements are located at 42 CFR 441.301(c)(1)(vi).
Conflict of Interest Defined
Providers of HCBS for the individual, or those who have an interest in or are employed by a provider of HCBS for the individual must not provide case management or develop the person–centered service plan.
Exception: Where the State can demonstrate that the only willing and qualified entity to provide case management and/or develop person–centered service plans in a geographic area also provides HCBS.
In these cases, the State must devise conflict of interest protections including separation of entity and provider functions within provider entities, which must be approved by CMS. Individuals must be provided with a clear and accessible alternative dispute resolution process.
In addition, certain NHTD and TBI services are NOT subject to COI.
Source: 42 CFR 441.301, Subpart (c)(1)(vi)
| NHTD Waiver Services | TBI Waiver Services | ||||
|---|---|---|---|---|---|
| Exempt Services | Non–Exempt Services | Exempt Services | Non–Exempt Services | ||
| Assistive Technology (AT) | Service Coordination | Independent Living Skills and Training | Assistive Technology (AT) | Service Coordination | Independent Living Skills and Training (ILST) |
| Moving Assistance | Community Integration Counselling (CIC) | Structured Day Program Services | Community Transitional Services (CTS) | Structured Day Program Services | Positive Behavioral Interventions and Support Services (PBIS) |
| Community Transitional Services (CTS) | Nutritional Counseling/Educational Services | Transportation Services | Environmental Modifications (E–Mods) | Substance Abuse Program Services | |
| Congregate and Home Delivered Meals | Peer Mentoring | Wellness Counselling | Transportation Services | ||
| Environmental Modifications (E–Mods) | Positive Behavioral Interventions and Support Services (PBIS) | Home and Community Support Services (HCSS) | Community Integration Counselling (CIC) | ||
| Respiratory Therapy | Home Visits by Medical Personnel | Home and Community Support Services (HCSS) | |||
| Respite | Respite | ||||
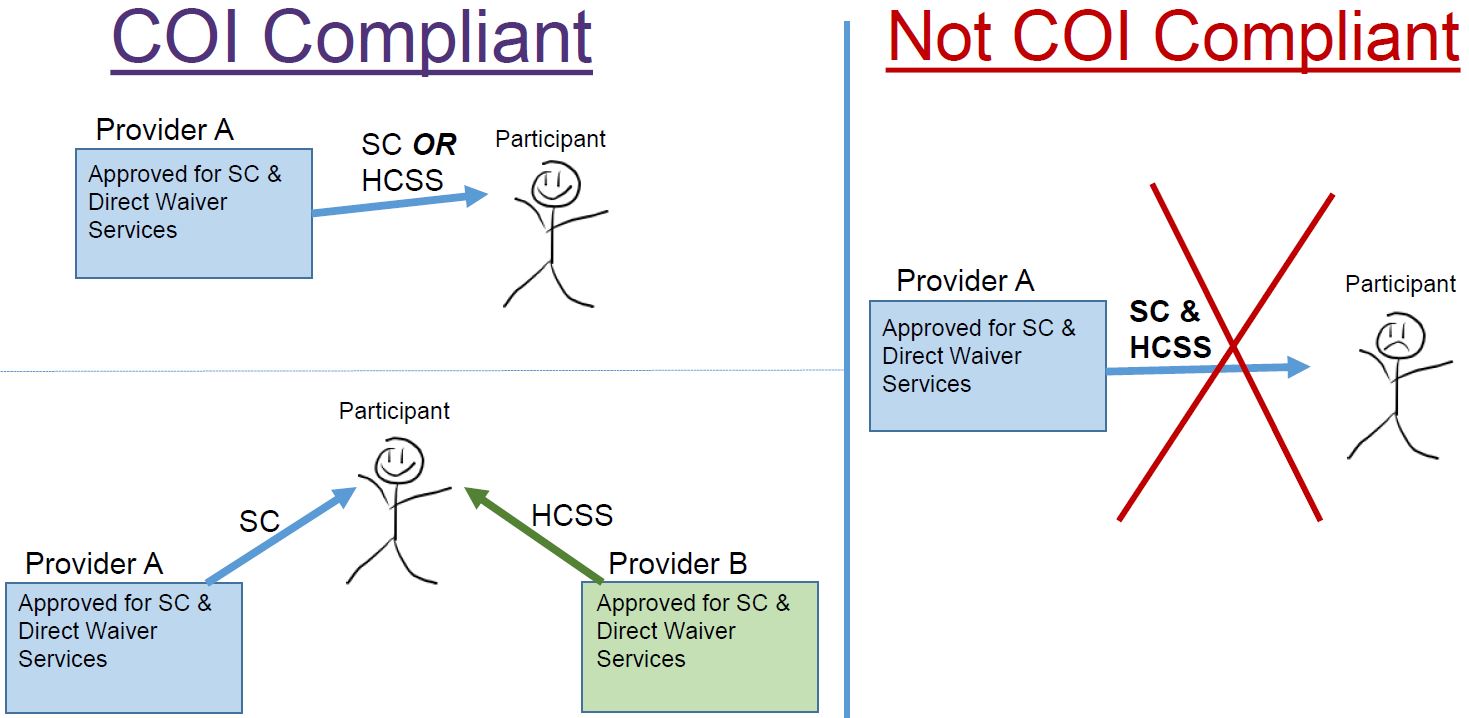
Conflict of Interest Compliance
- The HCBS Final Rule is focused on the individual/participant not the provider.
- The individual may not receive service coordination (i.e., case management/planning) and direct waiver services from the same provider.
- Therefore, the rule does not necessarily preclude providers from offering both service coordination and other direct waiver services.
High Conflict of Interest Providers
- A high conflict of interest provider is one in which at least 50% of the Service Coordination caseload also receives HCSS from the agency.
- 20% of current TBI providers are considered to be "high conflict" providers.
- 30% of current NHTD providers are considered to be "high conflict" providers.
- It should be noted that TBI has at least one HCSS provider in every region that does not provide Service Coordination. NHTD has seven regions that meet this criterion. This data warrants further consideration.
Based on claims data.
69% of NHTD Service Coordination Providers Also Provide Other Direct Services
| NHTD 2018 | |||||
|---|---|---|---|---|---|
| Region | Total # of Approved Providers | # of SC + Other Services (not exempt*) Providers | # of SC + Other Services (exempt*) Providers | # of SC only Providers | # Non#8211;SC Services Only |
| Adirondack | 23 | 15 | 1 | 0 | 7 |
| Binghamton | 26 | 18 | 2 | 2 | 4 |
| Buffalo | 13 | 8 | 0 | 0 | 5 |
| Capital | 21 | 12 | 0 | 0 | 9 |
| Long Island | 35 | 23 | 0 | 2 | 10 |
| Lower Hudson Valley | 35 | 24 | 2 | 0 | 9 |
| New York City | 38 | 31 | 1 | 0 | 6 |
| Rochester | 25 | 19 | 1 | 1 | 4 |
| Syracuse | 20 | 13 | 0 | 0 | 7 |
| Total | 236 | 163 | 7 | 5 | 61 |
*Exempt Services include: AT, CTS, Moving Assistance, Congregate/Home Delivered Meals and e–Mods/Vehicle Mods
Source: Conflict of Interest Compliance Implementation Plans
67% of TBI Service Coordination Providers Also Provide Other Direct Services
| TBI 2018 | |||||
|---|---|---|---|---|---|
| Region | Total # of Approved Providers | # of SC + Other Services (not exempt*) Providers | # of SC + Other Services (exempt*) Providers | # of SC only Providers | # Non#8211;SC Services Only |
| Adirondack | 27 | 17 | 0 | 0 | 10 |
| Binghamton | 34 | 21 | 1 | 2 | 10 |
| Buffalo | 18 | 11 | 0 | 0 | 7 |
| Capital | 25 | 12 | 0 | 0 | 13 |
| Long Island | 36 | 22 | 1 | 2 | 11 |
| Lower Hudson Valley | 36 | 28 | 0 | 0 | 8 |
| New York City | 36 | 30 | 0 | 0 | 6 |
| Rochester | 23 | 19 | 0 | 1 | 3 |
| Syracuse | 32 | 18 | 0 | 0 | 14 |
| Total | 267 | 178 | 2 | 5 | 82 |
*Exempt Services include: AT, CTS, and e–Mods/Vehicle Mods
Source: Conflict of Interest Compliance Implementation Plans
Potential Exemptions from COI
- An exemption may be granted if the State can demonstrate that the only willing and qualified entity to provide case management and/or develop person–centered service plans in a geographic area also provides HCBS.
- For example:
- Rural/frontier area "naturally" limits pool of available entities;
- Cultural considerations; and
- Linguistic considerations.
- CMS requires supporting documentation for any request for exemption.
Recent COI Survey
- The Conflict of Interest Survey via SurveyMonkey© was distributed on January 3, 2019.
- The survey collects county data by waiver services, including Service Coordination, and inquiries about capacity to serve new waiver participants.
- This data will help us determine if there are exemptions under the "only willing and qualified" provider criteria.
- As of January 9, 2019:
- NHTD received 47 responses
- TBI received 52 responses
- Average survey completion time: 4 – 7 minutes
- Not enough surveys have been completed for the data to generate a definitive analysis.
Considerations for Developing Potential COI Compliant Service Models
- HCBS providers cannot provide case management or person–centered planning for people on their caseload.
- Under our current waivers, both functions (case management and person–centered planning) above fall under Service Coordination.
- If there is only one willing and qualified HCBS provider in a geographic region, that HCBS provider may provide case management to and/or develop the person–centered plan for people on their caseload as long as conflict of interest protections are in place.
- CMS has approved the State´s request to exempt Assistive Technology, Environmental Modifications, Vehicle Modifications, Moving Assistance and Congregate/Home Delivered Meals from COI requirements. Providers who offer Service Coordination may also provide these services to the same participants.
- For the NHTD and TBI Waivers, the State is obligated to:
- Offer informed choice regarding services and supports that the participant receives and from whom;
- Include a mechanism for the participant to request updates and amendments to their service plan;
- Reflect the cultural consideration of the individual;
- Ensure continuity of care;
- Provide necessary information and support to ensure the individual directs the person–centered planning process; and
- Provide services in an HCBS–compliant setting.
Potential Service Models
- Service Coordination separation model*
- Providers continue to provide multiple services but cannot provide service coordination and other direct waiver services to the same individual.
- Functions of Service Coordinators (SCs) may remain the same.
- An individual´s SC cannot be employed by a provider who is also offering direct waiver services to that individual.
- Service Coordination only providers and those who offer Service Coordination and other exempt services may continue business as usual.
- DOH/RRDC maintains authority over provider designation and final plan approval.
- Providers continue to provide multiple services but cannot provide service coordination and other direct waiver services to the same individual.
*Cultural and rural exemptions still apply.
Potential Service Models
- Statewide organization model*
- A statewide organization provides Service Coordination only.
- Service Coordination provider enrollment is limited to statewide Service Coordination agency/agencies.
- Service Coordination only providers and those who offer Service Coordination and other exempt services may continue business as usual.
- The provider(s) offer no other direct waiver services.
- A statewide organization provides Service Coordination only.
*Cultural and rural exemptions still apply
|top of section| |top of page|Discussion and Other Suggestions for COI Compliant Models?
Timeline for Implementation
- The Corrective Action Plan (CAP) is the formal agreement with CMS on the activities and timelines the state will engage in to meet the COI requirements. The approved CAP authorizes the state to continue providing services pending full COI compliance.
- The NHTD and TBI waivers must be fully compliant (implemented and operational) with Conflict of Interest Provisions by January 1, 2021.
- Because we are under extension and not in compliance, CMS has required that DOH submit a revised CAP to reflect the January 1, 2021 date for compliance which is now under CMS review.
| Timeline to Compliance #8211; The Dates Below are Subject to CMS Approval | ||
|---|---|---|
| Compliance Readiness Action | Due Date | |
| 1. | Stakeholder workgroup/service model development period
|
Begins January 2019 |
| 2. | Ongoing CAP meetings with CMS | Ongoing |
| 3. | Submission and approval of final model to CMS
|
4/2019 30 days |
| 4. | Develop and implement transition steps
|
4/2019#8211;7/2019 |
| 5. | Communication of final transition plan and CAP status | 7/2019 |
| 6. | Federal public notice and public comment | 7/2019#8211;8/2019 |
| 7. | Submission and approval of waiver amendments | 9/2019#8211;12/2019 |
| 8. | Systems and edits development and implementation (eMedNY) | 4/2019#8211;1/2021 |
| 9. | Final transition and full compliance with COI | 1/2020#8211;1/2021 |
Next Steps
- Reconvene on:
- Results of Survey
- Stakeholder Feedback
- Meeting Date in February
Appendix
HCBS Settings Requirements
- Is integrated in and supports access to the greater community
- Provides opportunities to seek employment and work in competitive integrated settings, engage in community life, and control personal resources
- Ensures the individual receives services in the community to the same degree of access as individuals not receiving Medicaid HCBS
- Is selected by the individual from among setting options including non–disability specific settings
- Ensures an individual´s rights of privacy, respect, and freedom from coercion and restraint
- Optimizes individual initiative, autonomy, and independence in making life choices
- Facilitates individual choice regarding services and supports and who provides them
*There are additional standards for provider–owned and/or controlled settings
Provider–Owned and Controlled Standards
In such settings where the HCBS provider owns or operates the HCBS recipient´s residential service, the additional standards below apply:
- The additional standards for residential settings are:
- Individuals in residential units have legally enforceable agreements giving them the same protections and responsibilities as any tenant living in that jurisdiction
- Privacy in sleeping or living unit
- Units have lockable entrance doors
- The individual served, and appropriate staff have keys/codes to doors
- There is a choice of roommates in shared units
- Freedom to furnish and decorate sleeping or living units
- The additional standards for all settings are:
- Freedom and support to control one´s own schedule and activities
- Access to food and visitors at any time
- The setting is physically accessible to the individual (*not modifiable)

Follow Us