Thinking Differently About Person-Centered Planning
Money Follows the Person State Technical Assistance Project Presenter: Mary Lou Bourne, Director of NCI and Quality Assurance NASDDDS
- Document is also available in Portable Document Format (PDF)
Centers for Medicare & Medicaid Services (CMS)
New Editions Consulting, Inc.
Money Follows the Person (MFP)
Person-Centered Planning: Today´s Agenda
- A Brief look at the History and Fundamentals of Person-Centered Planning and Person-Centered Practice
- CMS Final Rule on Person-Centered Planning for HCBS 1915 (c) and (i)
- The Core Concept - What is important TO the person is different from what is important FOR the person.
- A system in place to support person-centered planning to make transitions successful
- Providers of Service and Outcomes/Goals in Person-Centered Service Plans
A Brief History of Person-Centered Planning Development
- 1950´s - Carl Rogers develops patient-centered therapy
- 1978 - Planetree Health introduced patient-centered care
- 1980 - Jack Yates develops the Individual Service Design
- 1987 - Beth Mount publishes Personal Futures Planning
- 1989 - Marsha Forest and Evelyn Lusthaus publish MAPS and Circles
- 1992 - Michael Smull and Susan Burke Harrison formally launch Essential Lifestyle Planning (ELP)
- 1994 - Dr. Bill Thomas starts the Eden Alternative nonprofit
- 1995 - Jack Pearpoint, John O´Brien and Marsha Forest publish PATH
- 2001 - ELP develops Person Centered Thinking Tools
- 2003 - First Green House Project Home started
- 2011 - CMS published NPRM for HCBS included Person-Centered Planning for 1915(c) and 1915 (i)
- 2014 - CMS Final Rules published which address Person-Centered Planning for home and community-based services
Person-Centered Thinking, Planning and Practice– An Evolution Over the Years
- Person-centered thinking helps to establish the means for a person to live a life that they and the people who care about them have good reasons to value.
- Person-centered planning is a way to assist people who need HCBS services and supports to construct and describe what they want and need to bring purpose and meaning to their life.
- Person-centered practice is the alignment of service resources that give people access to the full benefits of community living and ensure they receive services in a way that may help them achieve individual goals.
Dispelling Myths– The Old Reputation of Person-Centered Planning
- Person-centered planning requires long meetings
- Using first person in a treatment or care plan makes it person-centered
- Person-centered planning only addresses the “fluff”, the soft goals not the tough stuff (issues of health and safety).
- The team develops a person-centered planning plan once, and then it´s done
- A facilitator must be graphically gifted to develop a person-centered plan
- Person-centered planning is fantasy, unrealistic goals that have no place in publicly funded service systems.
In fact it is a set of simple, respectful, easily communicated ways to address quality of life and health and safety goals together…
Person-Centered Thinking
- Basic point of reference is what matters most to the person, not to you as the professional
- Everyone has value, and deserves engagement that is dignified and respectful, no matter what their condition
- Underlying belief that the person´s life provides the context that must be the basis of planning
- The person is the expert in their own life
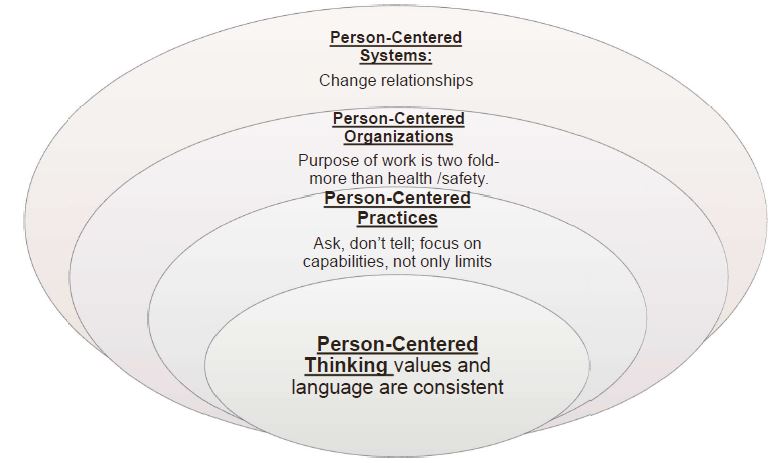
Person-Centered Thinking Leads to a Person-Centered System
- Each person involved in delivery support or services to eligible beneficiaries having their own set of core values leads to
- The language used, which leads to
- Decisions made and actions taken, which leads to
- Results and corresponding reactions
- Taken altogether, this becomes a continuous system of thinking and acting in a manner consistent with person-centered thinking
The Integration of Person-Centered Planning and Thinking
Person-centered planning, without person-centered thinking throughout the system, results in better paper or files, but not necessarily better lives.
Person-Centered Planning and Home and Community-Based Medicaid Authorities
Current Status with Medicaid Authorities
All Medicaid Home and Community-Based Services must adhere to person centered planning requirements.
- 1915(c) Home and community-based services waiver applications
- 1915(i) State Plan Amendment for home and community-based services
- 1915(j) State Plan Amendment for self-directed personal assistance services
- 1915(k) State Plan Amendment for Community First Choice Option
- 1115 Research and Demonstration projects
Person-Centered Service Planning Within Final Rule 42CFR 441.301 (c)(1)
- The person-centered planning process is driven by the individual
- Includes people chosen by the individual
- Provides necessary information and support to the individual to ensure that the individual directs the process to the maximum extent possible
- Is timely and occurs at times/locations of convenience to the individual
HCBS Person-Centered Planning: Steps
The person-centered plan process has 5 steps:
- Independent evaluation and determination of eligibility (for state plan services)
- An independent assessment of need (for state plan services)
- The person centered service planning meeting
- Writing the person-centered service plan
- Reviewing the plan
Perhaps the Most Overlooked Clause Related to Person-Centered Planning:
441.301 (c) (2) The Person-Centered Service Plan.
- "The person-centered service plan must reflect the services and supports that are important for the individual to meet the needs identified through an assessment of functional need, as well as what is important to the individual with regard to preferences for the delivery of such services and supports. Commensurate with the level of need of the individual, and the scope of services and supports available under the State´s 1915(c) HCBS waiver, the written plan must…"
The Plan Document: Some Key Elements
- Identifies:
- – the strengths, preferences, needs (clinical and support), and desired outcomes of the individual
- The plan also includes risk factors and plans to minimize them
- Is signed by all who implement the plan, and the person whose plan it is
Written plan reflects –
- Setting is chosen by the individual and is integrated in, and supports full access to the greater community
- Opportunities to seek employment and work in competitive integrated settings
- Opportunity to engage in community life, control personal resources, and receive services in the community to the same degree of access as individuals not receiving Medicaid HCBS
Both the Person-Centered Plan and the Process to Develop it:
- Assist the person in achieving personally defined outcomes in the most integrated community setting, and it is written to ensure delivery of services in a manner that reflects personal preferences and choices, and
- Contributes to the assurance of health and welfare.
- Reflects cultural considerations
- Uses plain language
- Includes strategies for solving disagreement
- Offers choices to the person regarding services and supports the person receives and from whom
- Provides a method to request updates
Person-Centered Service Plan Modifications
- Any modifications to the HCBS settings requirements needed by an individual must be supported by a specific assessed need and justified in the person-centered plan
- The following must be documented in the plan:
- Identify a specific and individualized assessed need
- Positive interventions and supports used prior to modification
- Less intrusive methods tried
- Describe the condition that is directly proportionate (commensurate) to the specified need
- Regular collection and review of data to review effectiveness
- Established time limits for periodic review to determine if modification is still needed
- Informed consent of the individual
- Assure interventions and supports will cause no harm
HCBS: Informed Choice
- 441.301 (C) (2) (ix) the plan must "Be finalized and agreed to, with the informed consent of the individual in writing, and signed by all individuals and providers responsible for its implementation."
- 1915 (c) HCBS Waiver application, Appendix B-7 Freedom of Choice
- A state must inform the person of the feasible alternatives under the waiver so that the individual (or the person´s legal representative) can make an informed choice.
- Informed: not just "told" – "informed" expects that people understand the differences and understand the implications and impact of the different choice.
- Choices require that options offered be desirable– meet the preferences and needs of the individual
A Few Differences About Person-Centered Planning
- Setting and circumstances matter
- Sequence matters (talk about preferences and values FIRST)
- Building on gifts and talents and natural support is different from fixing what is wrong and starting with the premise that professional support is best
- The degree of effort invested in planning is equal to the degree of support requested
- Nothing about me without me, and…
- Friends and families and those who love us and know us best can be equally as important as professional care givers in the plan development process, but participant selection is confirmed by the person who requires support.
Important TO and Important FOR: The Core Concept
It Begins With Learning How People Want to Live Their Life: What´s Important TO
What is important to a person includes what results in feeling satisfied, contcent, comforted, fulfilled, and happy.
- Relationships (people to be with)
- Status and control (valued role)
- Rituals & routines (cultural and personal)
- Rhythm or pace of life
- Things to do and places to go (something to look forward to)
- Things to have
Within That Context, Important FOR is Addressed
What others see as necessary to help the person
- Be valued (social rules, laws)
- Be a contributing member of their community (citizenship)
Issues of health
- Prevention of illness
- Treatment of illness/medical conditions
- Promotion of wellness (diet, exercise, sobriety)
Issues of safety
- Environment
- Wellbeing (physical and emotional)
- Free from fear (threats, abuse)
Person-Centered Planning is Not Either/Or
- Good person-centered planning that is well implemented eliminates many behavioral challenges and diminishes risk, especially when linked with positive interventions.
Those who write and implement plans must avoid the trap of "either/or" that is: happy or safe.
An effective person-centered plan assures BOTH/AND Both happy and safe
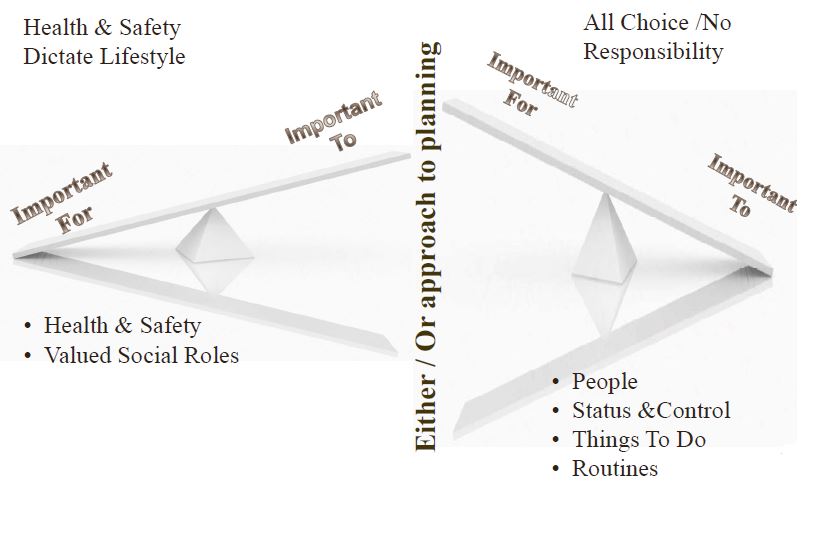
Effective Person-Centered Planning Describes the balance
Important For
- Health & Safety
- People
- Valued Social Role
Important To
- Status & Control
- Things To Do
- Routines
Care Plans Compared with Person-Centered Plans in Home and Community Based Services:
Traditional Care Planning
- Focus is on treatment or support for a medical diagnosis– assessing and addressing needs
- Goals often are identified by professionals
- May be developed without the person involved, then "reviewed" with the person present.
- Typically completed in one session, but can be iterative
- Reviewed at fixed intervals and changed when necessary to reflect response to treatment and progress toward goals
- Support section is directive about goals for staff to accomplish
Person-Centered Planning
- Focus is on how the person wants to live, with support necessary to achieve the desired life (their preferences and values)– building on gifts, abilities, and control
- Desired outcomes of the support are identified by the person and their loved ones
- The person and their closest family or friends actively participate in the full development
- It evolves over time, with support and preferences changing as the person changes
- Aim is to achieve a balance between personal preferences and health/safety/social rules.
Example
Alicia – transitioning back home
What´s important to Alicia – Relationships, Status and things to do
- Spending time with her family --- on the phone, in person, on the weekends; eating at least one meal each day with her husband
- Having opportunities to learn, to read new topics, and to develop new ideas;
- Spending time helping young people learn something new; helping other people.
- Practicing her faith, for a few minutes every day; for several hours every Sunday
- Staying connected to longtime friends- and talking politics with them.
- Coffee every morning, before she talks to anyone!!
- Relaxing with a good movie once a week (at least!)
What´s important FOR Alicia – health safety and valued social roles:
- Keeping her apartment clean so that she avoids respiratory infections– food put away and bathroom clean
- Putting things away, and removing clutter from her apartment so that she doesn´t fall
- Taking her daily medications as prescribed by her doctors (Seroquel, Lisinopril, metformin)
- Paying her bills on time, and letting others help her with her budget and checking account
- Transportation to her doctor appointments, and to see her husband in the Nursing Home
Integrating Person Centered Planning into the Community-Based Service System
Person-Centered Thinking to Systems
Person-Centered Planning Requires a Consistent Approach Throughout the Person-Centered System

What Comes Next: Upcoming Webinars will Address These Topics:
- Further exploration of person-centered planning regulations potential impact on location, type of home and desired outcomes for those who transition out of facility-based services
- Provider implementation of person-centered practices
- Outcomes in plans – how to measure progress
- What is an effective person-centered planning meeting?
- What can a state measure to determine the presence or absence of person-centered planning?
Further information can be found at these links:
- https://www.medicaid.gov/medicaid/hcbs/downloads/system-wide-person-centered-planning.pdf
- https://www.medicaid.gov/medicaid-chip-program-information/by-topics/waivers/downloads/technical-guidance.pdf
- https://www.medicaid.gov/medicaid/hcbs/downloads/faq-planned-construction.pdf
Contact: Roger Auerbach, MFP TA Team
Lead (RogerAuerbach@yahoo.com)
References By Slide
- Slide 14 - Person-Centered Service Plans Within Final Rule
42CFR 441.301 (c)(2) - Slide 15 - For a complete set of required written elements, refer to the rule:
42CFR 441.301 (c)(2)(i-xiii) - Slide 16 - Person-Centered Service Plans Within Final Rule
42CFR 441.301 (c)(1)(i-ix) and 441.301(c)(2)(i-xiii) - Slide 17 - Person-Centered Service Plans Within Final Rule
*42CFR 441.301 (c) (2) (xiii)

Follow Us